Article Text

Statistics from Altmetric.com
Antimicrobial resistance (AMR) has quietly become a global health crisis, claiming 1.1 million lives annually as of 2021. If left unchecked, the death toll is forecasted to climb to 1.9 million per year by 2050.1Despite the mounting volume of data on the burden of AMR, the global response has been sluggish with limited progress.
Global leaders agree that multi-sectorial and multi-faceted approaches are needed to limit the emergence and spread of AMR. Antimicrobial use is a key driver of AMR, where as much as 50% of use is unnecessary.2 3 In humans, the vast majority of antimicrobial use occurs outside of hospitals, making this setting crucial for antimicrobial stewardship efforts. With the estimated number of global outpatient treatment courses of antimicrobials in the billions,4 curtailing inappropriate prescribing is a daunting task. However, audit and feedback has a robust evidence base and offers hope as a scalable and impactful intervention to encourage practice change.
Audit and feedback (A&F) is an implementation strategy which measures and provides feedback on an individual’s practice in comparison to similar peers or accepted targets. The goal is to improve the quality of healthcare patients receive by encouraging providers to align with professional standards.5 A&F is supported by hundreds of trials across thousands of prescribers. Yet despite its documented efficacy in improving the quality of care, the intervention is sporadically implemented and too often voluntary in nature.
In this issue of BMJ Quality and Safety, Carney and coinvestigators present data from a large cluster randomised controlled trial using audit and feedback with peer comparison to improve antimicrobial prescribing for uncomplicated lower urinary tract infections (UTIs) and increase prescribing of the first-line agent—nitrofurantoin.6 The study randomised over 5000 family physicians to one of three arms—(1) audit and feedback providing individualised data on the proportion of first-line antibiotic selection compared with other family doctors in the province with local antibiogram data, along with an evidence summary describing the best practices for treatment of uncomplicated UTI, (2) an evidence summary alone or (3) neither. The combined A&F with educational summary, compared with the control group that received neither intervention, led to a 4.8% increase in preference for nitrofurantoin (OR 1.28, 95% CI 1.07 to 1.52), with a corresponding decrease in non-first line recommended antibiotics. During the 6-month study period, an additional 8.7 cases of UTI per 100 family physicians were prescribed nitrofurantoin compared with potentially less effective or more toxic alternatives. The study did not find any significant impact of A&F with educational summary compared with education summary alone, highlighting the impact of A&F combined with relevant educational materials to guide behaviour change.
Antibiotic prescribing is a complex behaviour. It is influenced not only by prescriber knowledge but also their motivation (eg, fear of negative consequences when antibiotics are not prescribed) and contextual factors (eg, perceived patient and family pressure to prescribe antibiotics).7 8 Further, antimicrobial prescribing represents various decision nodes: (1) initiation—does this patient have an infection that would benefit from an antimicrobial?; (2) selection—if so, which antimicrobial, dosage and frequency is optimal? and (3) duration—how long to treat to cure the infection but also reduce the risk of side effects and limit the emergence of AMR?
All antibiotic prescribing decision nodes can be influenced by A&F; however, initiation represents both the most complicated behaviour change decision node as well as the most impactful for patient care and public health. Therefore, we recommend antibiotic initiation be the preferred target for A&F. Well-designed feedback interventions which focus on total volume or unnecessary antibiotic prescribing can impact initiation.9 10 Selection and duration decision nodes are commonly related to knowledge gaps for physicians and are more amenable to change through educational initiatives alone. In the study by Carney et al, the focus is on antibiotic selection, whereby a small but significant improvement in appropriate prescribing was noted with A&F and evidence summary. However, even in the group receiving the evidence summary alone, a 3.3% absolute increase in appropriateness was seen (OR 1.17; 95% CI 0.99 to 1.38), demonstrating a small impact of education as a sole intervention.
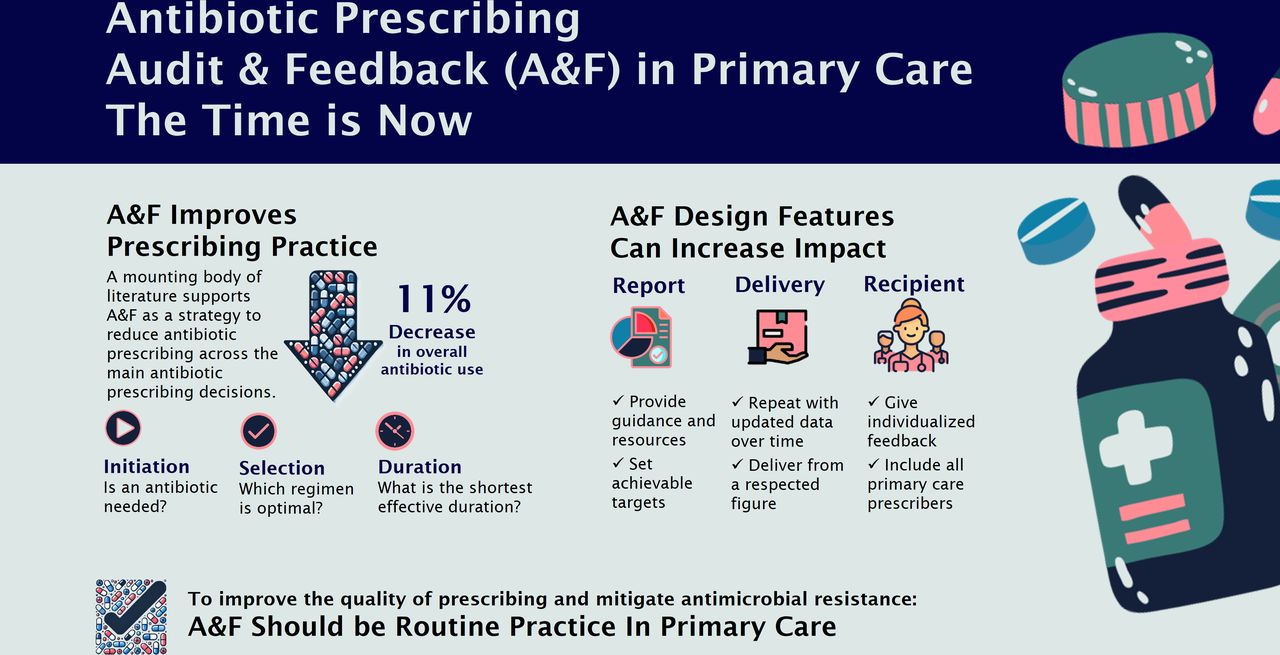
This study contributes to a mounting body of high-quality research supporting A&F as a method to improve the appropriateness of antibiotic prescribing. An recently published systematic review and meta-analysis11 evaluating A&F shows its significant impact on antibiotic prescribing in primary care across all decision nodes. Across 56 randomised controlled studies and 36 547 prescribers or clinics, A&F led to an 11% relative reduction in antibiotic prescribing volume, 23% reduction in unnecessary antibiotic initiation, 17% reduction in broad-spectrum antibiotic selection and 13% reduction in prolonged antibiotic duration. There was substantial between-trial heterogeneity; not all studies had a similar impact on prescribing, and some had none at all. This variability reinforces the need to carefully design A&F interventions and employ feedback strategies that are most likely to influence change. Experts suggest a variety of factors influence the effectiveness of A&F interventions.12 13 Considerations include the content of the feedback (eg, connecting the data to desired behaviour change, includes clear direction on how to change behaviour), the delivery of the feedback (eg, including a clear graphic, the frequency and timing of the feedback) and the recipient themselves (eg, the extent to which behaviour is under the provider’s control).14 Figure 1 describes key considerations related to implementing A&F for antibiotic prescribing in primary care.

{kind=link}
Considerations for antibiotic audit and feedback implementation in primary care.
A&F can make a small but significant dent in the 30–50% of antibiotics that are inappropriately prescribed. But this leaves a lot of room to move the needle further. There is still work to do to better understand how best to design A&F for each decision node, across different healthcare contexts and identify the mechanisms by which this approach influences change. Comparing A&F to no intervention will likely yield limited additional scientific value.5 Further research is needed on how best to engage busy clinicians to attend to A&F, as well as using behavioural science to maximise the impact of A&F delivery. To further improve the quality of prescribing, particularly to reduce unnecessary initiation of antibiotics, evidence-based cointerventions can be combined with A&F and act on other barriers and facilitators to change. The US Centers for Disease Control and Prevention provides a list of Core Elements of Outpatient Antibiotic Stewardship which offers a holistic framework for effective stewardship in primary care and potential strategies for cointerventions.15 The core elements include Commitment (eg, public commitment posters16 attesting to judicious prescribing), Action (eg, accountable justification9 when prescribing antibiotics for acute respiratory tract infections, public communication campaigns17), Tracking and Reporting (eg, A&F with peer comparison) and Education and Expertise (eg, guideline dissemination, communication skills training).18
While we further hone these feedback strategies, the evidence is clear—A&F works. We urge health system leaders and policy-makers to take decisive steps to integrate A&F into the healthcare system on a non-voluntary basis to help reduce inappropriate antimicrobial prescribing and mitigate the emergence of resistance. For example, in Ontario, Canada, we combined a voluntary electronic dashboard with a mailed antibiotic A&F letter (with an opt-out option) as part of a randomised trial, successfully reducing antibiotic prescribing.10 We are planning to continue with the success of this programme to reach all prescribers in a quality improvement initiative. A successful A&F programme requires interdisciplinary collaboration between policy-makers, data scientists, subject matter experts, professional organisations and patient partners to develop a system to deliver impactful and sustained messaging. When A&F is stopped, the impact on prescribing wanes —so the implementation of an ongoing programme with repeated messaging is key.19 Meanwhile, the onus is on antimicrobial stewards and researchers to refine these strategies, determine novel ways to improve prescribing across each decision node and evaluate their impact on patient and population outcomes. With immediate action, A&F can play an important role in mitigating the threat of AMR.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
X @BRxAD, @@DrKevinSchwartz
Contributors BL: conceptualisation, writing—original draft, guarantor. KS: conceptualisation, writing—reviewing and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.