Article Text

Abstract
Introduction Health education, weight control and exercise therapy are recognised treatment options for the non-surgical management of knee osteoarthritis (KOA); however, the pain and muscle fatigue associated with exercise make it difficult for patients to initially adhere. Traditional Chinese medicine (TCM) massage is an important complementary and alternative therapy that can effectively address these deficiencies. According to TCM theory and preliminary clinical practice, loosening of the muscles while pointing to acupoints can promote the recovery of KOA. Therefore, we hypothesised that exercise therapy in conjunction with TCM massage may lead to more satisfactory results in terms of pain management, active functional muscle activation patterns and proprioception in patients with KOA.
Methods and analysis A parallel, single-centre, randomised controlled trial involving 106 patients will be conducted at Shuguang Hospital, Shanghai University of Traditional Chinese Medicine. Eligible patients with KOA who agree to participate will be randomised via a 1:1 randomisation system into the experimental group (receiving TCM massage and exercise treatment) and the control group (receiving exercise treatment). The primary endpoint is the change in the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) for pain from baseline to 24 weeks. Secondary outcomes include knee function (measured using the WOMAC stiffness and WOMAC functional subscale questionnaire and the timed ‘Up and Go’ test), muscle activation states (evaluated with electromyography techniques), knee proprioception and treatment satisfaction, adherence, safety evaluation and other relevant factors. Outcome assessors and data analysts will be blinded to the allocations, and the participants will not disclose their specific allocations. Outcome analyses will be conducted on both intention-to-treat and per-protocol populations. A preliminary analysis will test whether TCM massage, in addition to exercise, has statistically better outcomes.
Ethics and dissemination The study protocol has received approval from the Ethics Committee of Shuguang Hospital, Shanghai University of Traditional Chinese Medicine (2023-1357-124-01).
All study participants will be required to give written informed consent. The findings of the study will be submitted to a peer-reviewed journal for publication and presented at scientific conferences. Additionally, the participants will receive copies of the results.
Trial registration number ChiCTR2300077308.
- China
- REHABILITATION MEDICINE
- Musculoskeletal disorders
- Knee
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study will evaluate the long-term (24-week follow-up) therapeutic effects of traditional Chinese medicine (TCM) massage with exercise on knee osteoarthritis (KOA).
This study will demonstrate the effects of TCM massage therapy on the patient’s proprioception and degree of muscle recruitment.
It may provide initial therapeutic assistance for patients with KOA who have difficulty adhering to exercise therapy or who resist exercise therapy treatment.
This study includes patients with KOA in the Kellgren-Lawrence I—III classification and may not be generalisable to patients with severe KOA.
Only KOA patients with single knee involvement will be included in this study, and the effect on patients with KOA in both knees remains to be verified.
Introduction
Knee osteoarthritis (KOA) results in clinical manifestations, including pain, stiffness, swelling and functional limitations of the knee joint.1 About 240 million people suffer from symptomatic mobility-limited arthritis.2 According to data from the National Health Interview Survey and validated simulation models, there are 14 million individuals in the USA who have symptomatic KOA.3 A recent meta-analysis found that the overall pooled estimate of symptomatic KOA prevalence in China was 14.6%.4 KOA is one of the most common chronic health conditions, and patients with KOA suffer from arthritis-related limitations in daily activities, causing not only pain and limitations in physical function but also many other outcomes, affecting mental health, sleep, work participation and even mortality.5 KOA results in significant medical costs, with patients spending an average of approximately $15 000 on direct medical costs over their lifetime.6 The American College of Rheumatology and the Osteoarthritis Research Society International guidelines7 8 recommend a core set of programmes for non-pharmacological interventions for patients with KOA, including education, weight control and exercise, which have been recognised internationally. Among these, exercise therapy is ranked the best treatment for osteoarthritis pain.9 However, it is initially resisted by patients due to stiffness and pain in the knee joint, and the muscle soreness that results from the activity makes it difficult for older people to maintain long-term exercise therapy.10 It is important to seek a therapy that addresses these negative effects in the early stages of recovery from KOA.
Massage therapy, a complementary health approach, is used by approximately 15.4 million people in the USA.11 Massage therapy with relaxation effects12 can play a role in releasing adhesions and activating and regulating muscle function, which can improve the clinical outcomes of patients with KOA. Its main mechanism of action is the promotion of blood circulation and metabolism.13 A systematic review and meta-analysis suggested that massage therapy may be effective and safe for improving pain, stiffness and physical function in patients with KOA as a complementary and alternative therapy.14 Some early randomised controlled trials on the effectiveness of massage for KOA concluded that massage reduces pain and improves knee mobility.15 16 Massage therapy may provide more multifaceted advantages and potential in the treatment of KOA, such as proprioception and patient satisfaction; however, this has rarely been reported by researchers. Therefore, a randomised controlled trial investigating the multidimensional benefits of massage therapy as an intervention for KOA is warranted.17
Muscle activation determines the knee joint loading.18 Surface electromyography (EMG) uses electrodes placed on the skin to record the electrical activity that causes muscle contractions (ie, muscle action potentials) and provides important information about the peripheral properties and central strategies of the neuromuscular system.19 EMG-driven modelling studies have shown that muscle strength contributes significantly to knee joint loading.20 Increased KOA severity results in increased muscle activation compared with that in patients with less severe disease.21 The muscle activation in KOA is synergistic. However, synergistic contraction stabilises the knee joint and maintains strength but also pushes and pulls on the femur and tibia, unbalancing the force lines in the lower limb and altering the biomechanical characteristics, thereby exacerbating symptoms.22 It was suggested that older people with KOA or at risk of KOA may have adequate quadriceps strength; however, possibly due to excessive hamstring synergistic activation, quadriceps torque may be diminished and not focused on strengthening the quadriceps at the time of treatment because of excessive antagonist muscle activity.23 This provides a framework for new ideas in massage therapy for KOA and demonstrates the mechanism of action of massage therapy in terms of muscle activation patterns.
‘Tendons first’ is an important theoretical basis and guiding ideology for treating tendon and bone diseases in traditional Chinese medicine (TCM), which refers to the need to focus on soft tissues in the treatment of diseases using TCM massage. Using AnyBody simulation technology, we found that TCM massage therapy could inhibit overactivated muscles and promote optimal muscle activation.24 The technology is beneficial for the treatment of KOA, with a trend toward positive efficacy. As we grapple with the issue of the effects of massage on KOA, we have successfully conducted an observational study involving patients with KOA to examine the effects of TCM massage therapy on pain. Findings from this study suggest that TCM massage therapy is a useful complementary treatment and alternative therapy option for short-term pain relief in patients with KOA.25 TCM massage may change the biomechanical characteristics of these patients and help them recover walking ability. However, muscle activation of the lower limbs of patients with KOA using TCM massage still needs to be demonstrated through objective observation, and findings from such studies will be important in explaining the mechanism of muscle mechanics.
TCM massage can relieve muscle soreness and help patients with KOA recover from negative emotions and disabilities, producing better results.26 Combining massage therapy with exercise may improve the clinical outcomes in patients with KOA.27 Nonetheless, a systematic review found that there are very few studies that specifically examine whether this leads to higher outcomes and better compliance,28 and there is a lack of long-term efficacy and follow-up observations.29 It is of great significance to conduct a high-quality randomised controlled trial to objectively observe whether TCM massage can achieve better patient compliance and long-term efficacy than conventional treatment. Therefore, based on exercise therapy, we aim to design a deterministic trial that focuses on examining the effects of TCM massage therapy on pain, activity-function muscle activation patterns and proprioception in patients with KOA in the present study.
Objectives
To study the effects of TCM massage combined with exercise compared with exercise only on pain, functional activity and proprioception in patients with KOA.
To evaluate the long-term efficacy and patient satisfaction with TCM massage combined with exercise in the treatment of KOA.
To observe changes in the lower limb muscles during activity in patients with KOA due to TCM massage in an attempt to explain the mechanical mechanism of action of TCM massage.
Methods and analysis
Study design and setting
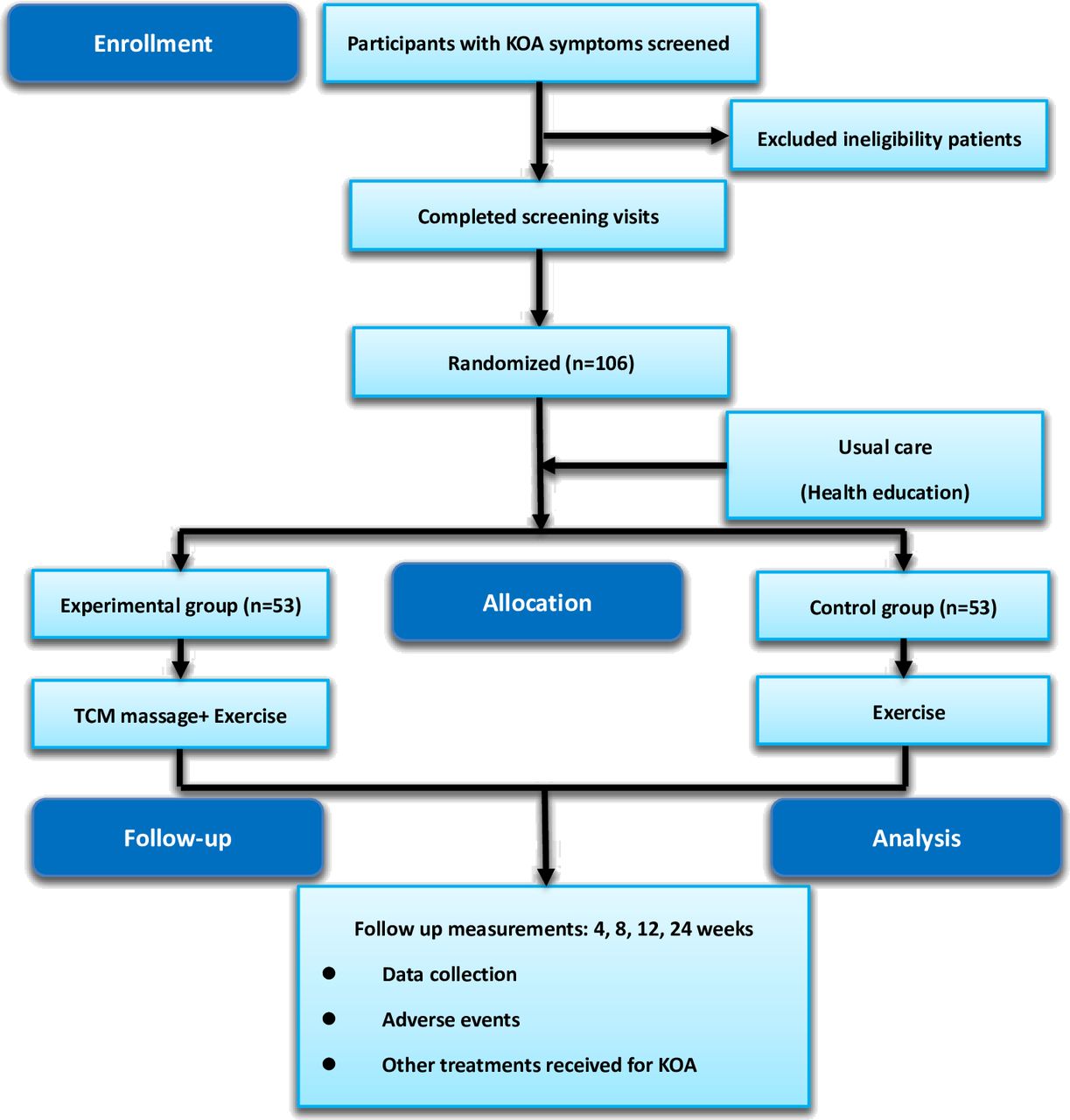
We followed the design, conduct and reporting of clinical trials on KOA to report our trial protocols. The study protocol was registered with the China Clinical Trial Registry (registration number: ChiCTR2300077308). The study will follow the rigorous standards outlined in the Declaration of Helsinki and the Standard Protocol Items: Recommendations for Interventional Trials.30 This study protocol was approved by the Ethics Committee of Shuguang Hospital, Shanghai University of Traditional Chinese Medicine (2023-1357-124-01). We plan to conduct a single-centre, randomised, parallel, controlled trial at the Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, which is a tertiary hospital. The study duration will be 24 weeks. Eligible and consenting 106 patients with KOA will be randomly allocated in a 1:1 ratio using a computer-generated random number to the experimental group (n=53) or control group (n=53) to receive treatment for 8 weeks. Participants will be assessed at baseline and at 4, 8, 12 and 24 weeks post-intervention to determine whether better long-term outcomes are achieved with TCM massage and exercise than with exercise alone. A flowchart of the study process is shown in figure 1. The timelines for patient enrolment, intervention and assessment are presented in table 1.

Trial design of the research procedure.
Study timeline for data measurement
Recruitment and informed consent
All participants will be recruited from the hospital and community. The trial will be designed with an open recruitment advertisement to recruit patients online or offline (eg, WeChat public website). Orthopaedic, TCM and rehabilitation physicians will strictly determine whether patients are eligible for this study based on the inclusion and exclusion criteria, and screening of participants will be conducted by a regular non-participant in the study. If the patients who are interested and volunteered to participate in this trial meet the inclusion criteria, they will sign a written informed consent form before the start of the study. All participants will receive nominal compensation (including a gift voucher for a future massage). Participants will be fully informed about the study, including its procedures, benefits and potential risks, except for information about other in-group interventions. They are free to withdraw from the study at any time without penalty or any negative impact on their future medical treatments.
Study population
Diagnostic criteria
We will include patients aged 50–80 years who meet the following diagnostic criteria of the American College of Rheumatology: knee pain on most days of the week with at least two of the following: stiffness for less than 30 min/day, crepitus, bony tenderness, bony enlargement and no palpable warmth.31
Inclusion criteria
Single knee pain.
Disease duration of at least 1 year.
Imaging evidence of tibiofemoral joint redundancy knee.
Moderate KOA (Grades I–III per the Kellgren-Lawrence criteria).32
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale score of >8/20.
Exclusion criteria
Physiotherapy for KOA pain in the past month.
Intra-articular injection of glucocorticoids or viscosupplementation in the past 6 months.
Serious mental, neurological, infectious, gastrointestinal, cardiovascular, immunological, respiratory or renal diseases.
Tumour, tuberculosis, rheumatoid arthritis, gout, lower limb sprain or trauma, or any other chronic pain condition.
Communication disorder.
Positive patellar float test.
Skin breaches around the knee.
Participation in other clinical trials of massage.
Removal criteria
Not meeting the inclusion criteria or misdiagnosed.
Serious adverse events or complications during the trial that preclude further study.
Unwilling to cooperate with treatment.
Request to withdraw from the study for personal reasons.
Randomization and blinding
The study will be randomised and parallel-controlled, with a separation of efficacy evaluators, patients and statisticians, and will not be blinded to the patients or physicians. Indicator evaluators and statisticians will be unaware of the subgroups, and therapists will be unaware of the outcome evaluation. The assessor will be blinded to follow-up outcome assessment. A random number table will be generated by a statistician using statistical software and distributed to third-party researchers for allocation concealment. Third-party personnel will place the numerical tables in opaque envelopes, each marked with a time and signature, and hand them uniformly to the study coordinator to ensure adequate randomisation concealment. The study coordinators will contact potential participants through telephone to inquire about their willingness to participate in the clinical trial. Individuals who meet the inclusion criteria will be invited to the biomechanics laboratory for baseline testing, where subjective scale scores, objective physical function data and biomechanical data will be recorded. Each participant’s sex and severity of condition will be collected. After completion of baseline testing, the participants will be allocated to the test and control groups according to random numbers on a 1:1 basis. Stratified randomised subgroups will be formed based on the order of random allocation using a block randomisation grouping method with block lengths set at two or four to ensure that patients in each group are matched for sex and severity of KOA.
Intervention
All patients will receive health education that includes awareness on KOA disease and treatment goals, explanations of issues related to joint loading and dosage of physical activity/exercise, encouragement on how to make healthy lifestyle changes by adopting behaviours that may have a beneficial effect on their condition or at least prevent worsening it, management of unexpected high-risk events, and advice on how to control their weight and maintain a normal weight.33 Details of the health education programme are displayed in online supplemental appendix 1.
Supplemental material
Experimental group
Patients in the experimental group will undergo an exercise programme and TCM massage. Considering the patients’ clinical symptoms and level of functioning, the exercise programme will be individualised to meet their specific needs. The exercise programme will be based on the American College of Sports Medicine guidelines on exercise for older adults, which encourages patients with KOA to be actively involved in exercise.34 The exercise goal is 50%–70% increasing in the heart rate reserve. Participants will engage in a total of 24 group training sessions of 20–30 min exercise three times per week for 8 weeks. Prescribed exercise programmes will include aerobic walking and resistance training of the affected limb.10 Information on pain level, local vs central sensitisation, range of motion and weight-bearing tolerance within the effective range of motion of the knee will be obtained from the patient’s past and present medical history and clinical physical assessment. This information will be used in the baseline setup of the exercise; the physical therapist selects a starting position (figure 2) and weight resistance that will be matched to the patient’s ability to perform two sets of 10 repetitions. To achieve the desired dose of exercise, there will be constant communication between the physiotherapists and the patient, and perceived exercise intensity (rate of perceived exertion) will be assessed at the completion of each exercise. The principles of self-reduced stress will be applied to ensure that the exercise is comfortable for the patient and is performed with little or no pain. The exercise logs include attendance, number of exercises, duration of each exercise, number of repetitions and number of sets. At the end of the exercise intervention period, the patients will be advised to maintain their normal daily activities.

Resistance training—guiding the patient to produce the correct quadriceps power pattern.
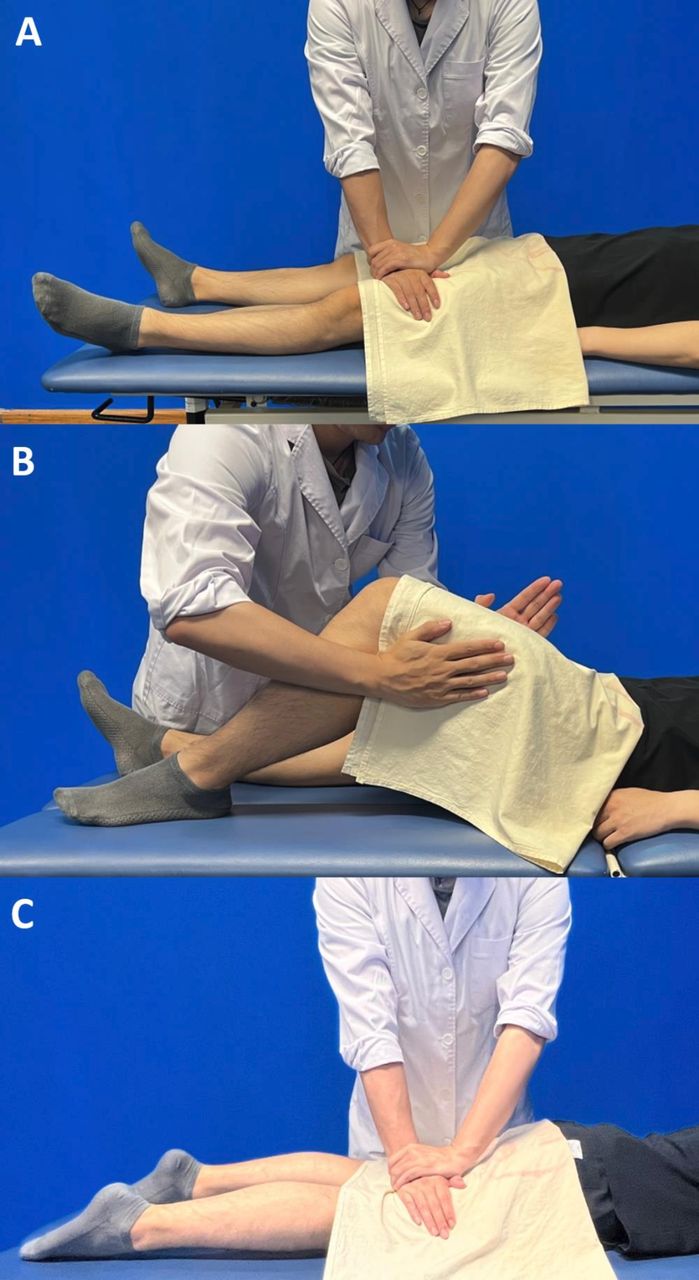
After the exercise programme is conducted, TCM massage treatment will be performed by licensed doctors from Shuguang Hospital with at least 3 years of clinical experience who have undergone specific training in tissue manipulation before the start of the trial. Prior to each treatment, the practitioner will check the patient’s current signs and adjust the massage intensity accordingly. After skin disinfection, the physician will press and relax the affected limbs (figure 3). The doctor will then apply superficial-to-deep pressure to the acupuncture points around the knee joint with the thumb to stimulate the acupuncture points and induce a localised sensation of soreness, distention or irradiation in patients who feel comfortable with the applied pressure. Each acupoint, including Liangqiu (ST34), Xuehai (SP10), Heding (EX-LE2), Dubi (ST35), Neixiyan (EX-LE4), Yinlingquan (SP9), Yanglingquan (GB34), Zusanli (ST36), Weizhong (BL40), Chengshan (BL57), Yingu (KI10), Ququan (LR8) and ashi point, will be pressed for 30 s (table 2). The treatments will be administered every alternate day for a week. The treatment sessions will last for approximately 30 min, and the entire intervention will last for 8 weeks.35

{kind=link}
{kind=link}
{kind=link}
Release massage techniques for the lower extremities.
Location of acupoints
Control group
Patients in the control group will undergo the same exercise programme as the experimental group only.
Concomitant medications
All patients will be advised to avoid using any other treatments, such as painkillers, glucocorticoids, other physical therapies, etc, for KOA during this period as much as possible through the informed consent form. However, if the patient had intolerable pain and the outcome was not assessed within the next 48 hours, the use of painkillers will be permitted. During the study, any other therapies used by patients to relieve KOA pain must be known to the researcher, who will record the therapy details, including the name of the treatment, dosage and duration.
At the first visit, participants will provide information on any other illnesses they currently have and the corresponding medications they use, all of which will be recorded in case report forms. All treatments administered will be recorded, including the name of the drug, its dose, the duration of treatment, and the start and end of dosing times.
Follow-up and outcomes
Knee pain, stiffness, active function, muscle recruitment and proprioception during walking, as well as patient satisfaction and treatment safety, will be measured at 4, 8, 12 and 24 weeks after randomisation of all participants.
The following measures will be taken to retain participants as much as possible: free medical consultation and guidance advice for other diseases without compromising KOA treatment; a daily schedule of optional treatment times and giving patients a 1-week notice to schedule their treatment for the week according to their schedule; adoption of a micro-appointment system with micro-text and phone calls to remind participants of upcoming treatments; and obtaining permission. The telephone numbers of the next of kin will also be recorded to facilitate follow-up.
Outcome assessments will be performed by a commissioner not involved in the intervention process and completed by the patients in a separate space in the outpatient department at each participating site. All outcome assessors will be trained in interviews and measurements before the start of the study and will follow a standard protocol.
Primary outcome
Womac pain subscale
The total score ranged from 0 to 20, with higher scores indicating greater pain. The pain categories on a 0–20-point scale are 0 (no pain), 2–8 (mild pain), 9–14 (moderate pain) and 15–20 (severe pain).36 The estimated minimum clinically important difference (MCID) between the groups using the half-standard deviation formula is 1.6.37
Secondary outcomes
Womac stiffness and womac functional subscale
Secondary outcomes included WOMAC stiffness (total score range, 0–8; higher scores indicated poorer function; MCID=2.4) and function score (total score range, 0–68; higher scores indicated poorer function; MCID=6), which assess the degree of difficulty with activities of daily living in the last 48 hours.38
The timed "up and go"
The timed up-and-go test is a valuable indicator of balance and general motor ability in older people and is a quick, meaningful and objective measure of functional mobility.39 It is widely used in many other neurological and neuromuscular disorders as well as in several other disease states; it has excellent internal reliability and very high retest reliability.40 It measures the time taken for the patient to stand up from the armchair, walk a distance of 6 m, turn around, walk back to the chair and then sit down, with more time taken indicating poor mobility.41
Emg data
EMG data will be collected from the affected limb using a Noraxon Ultrium surface EMG telemetry device (EMG software version: MyoResearch XP Basic edit on 6.59, EMG data acquisition frequency of 2000 Hz) manufactured by NORAXON (USA). The target electrodes will be mounted in the order of the MyoResearch software target electrode apparatus, defining odd numbers as left and even numbers as right, and labelling the target muscles according to numbers 1–6: medial femoral (ie, medial quadriceps), lateral femoral (ie, lateral quadriceps), biceps femoral (ie, lateral popliteal), semitendinosus and semimembranosus (ie, medial popliteal), medial gastrocnemius and lateral gastrocnemius muscles. The EMG signal from the gait test will be normalised to maximal voluntary contraction. Record the limb dynamics and muscle co-contraction in the gait of the patient while walking.42
Knee proprioception
Knee proprioceptive testing will be performed using an isometric muscle strength assessment training system (BIODE MEDICAL SYSTEMS, USA; Model: System 4 Pro).43 (1) Muscle force acquisition: the test protocol will be set for unilateral isometric centripetal exercise with an angular velocity of 60°/s at low speed and a cycle termination of 5 times as a reflection of the maximum muscle force of the muscles measured. The peak moments, peak moment ratios of the anterolateral homonymous muscle groups, and peak moment ratios of the ipsilateral flexors and extensors will be selected. The peak moment is the maximum moment output generated during muscle contraction. (2) Positional sensory acquisition/positional sensory perception: passive flexion of the knee will be done at a constant angular velocity starting from the fully extended knee position at 45° and 60° for 10 s to allow the patient to fully perceive. Active angular error: after returning to knee extension, patients will actively perform a knee flexion movement when they believe that the target angle has been reached; the movement will then be stopped, and the difference between the actual and target angles will be measured. The system automatically calculates the difference between the target angle and current angle for the active angle reproduction (AAR) value. The AAR will be used to evaluate knee position awareness, with a smaller AAR representing better position awareness.44
Treatment satisfaction
Patient satisfaction with rehabilitation will be collected at 4, 8, 12 and 24 weeks using a 20-cm Visual Analogue Scale anchored with ‘no satisfaction’ (0 cm) and ‘complete satisfaction’ (20 cm).45
Safety
To describe the distribution of adverse events, adverse reactions, significant adverse events and serious adverse events in participants and compare the incidence using the χ² test or Fisher’s exact probability method, we will tabulate the details of adverse events during treatment and analyse whether the adverse event was related to the treatment. Reporting of serious adverse events: all serious adverse events, whether related to the intervention or not, will result in immediate withdrawal of the patient from the trial, prompt treatment and reporting to the relevant unit within 24 hours.
Monitoring
To avoid atypical findings, each questionnaire will be reviewed before data entry and double-checked to be error-free before storing and backing up. Scale assessors will be professionals who are familiar with the study’s guiding phrases and entries and understand the meaning of all entries, to ensure correct interpretation. Problems identified during the assessment will be promptly addressed and resolved by the researcher. The scale will be administered in a quiet, comfortable environment. The purpose and precautions of the assessment will be explained to the participants before the assessment begins, and the assessment will be conducted entirely voluntarily. After completing the assessment, the researcher will check and supply missing items to ensure that the information is complete and accurate. The ethics committee and sponsor require that all relevant information should be recorded in the case files.
Patient and public involvement
Patients and the public are not involved in the development of the research questions or study design. They are not involved in recruitment, implementation or reporting of the study. The results of the study will be disseminated to study participants via social media.
Sample size
The effectiveness of TCM massage in the treatment of KOA was reported in a previous study26 to be approximately 60%. However, the proposed combination of TCM massage and exercise in this study is expected to increase the effectiveness by 25% (85% effectiveness). A completely randomised design estimated that 48 observations would be required in each group (P1=60%, P2=85%, α=0.05, β=0.20), and if 10% shedding was expected, 53 cases would need to be enrolled in each group, resulting in a total of 106 cases in two groups.
Statistical analysis
Excel 2019 (Microsoft) and Statistical Package for the Social Sciences (SPSS) Statistics V.25.0 (SPSS IBM) will be used to analyse the data. First, we will perform normality and variance χ² tests on the obtained data to determine the appropriateness of subsequent analysis. Continuous data will be expressed as mean±SD and IQR. For data that satisfied the normal distribution and variance χ² test, we will use t-tests to compare the differences in means between the groups. If the data are not normally distributed, non-parametric tests will be used. Categorical data will be expressed as percentages (n %), and baseline analysis will be performed using the χ² test or Fisher’s exact test.
The initial data analysis will be performed according to the intention-to-treat principle. Data of randomised participants, regardless of the actual treatment received, will be coded according to their allocation status. In preliminary analyses, to deal with repeated measures and account for inter-individual variability, we will use linear two-way analysis of variance (ANOVA) comparing outcomes at each time point between the two intervention groups, with time as a categorical variable to analyse the interaction between time and intervention at all time points except baseline, with age-stratified and sex-stratified factors as fixed effects, and with missing data supplemented with random interpolation. Secondary analyses will be performed using a conforming protocol analysis, including only participants who successfully completed the trial according to the intervention plan and did not receive any other treatment in the previous 4 weeks. During the analysis, we adjusted the p values for two-by-two post hoc comparisons using the Bonferroni method to control for statistical error rates. Additionally, Pearson’s correlation coefficients will be calculated to assess the strength of the association between secondary and primary outcomes.
Study duration
The trial recruitment period is 12 months, and it commenced in September 2023. The final participant was recruited in September 2024.
Ethics and dissemination
This study was approved by the Ethics Committee of Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, on 13 June 2023 (Approval Number: 2023-1328-95-01). Modifications of the protocol after the recruitment of the first participant were not permitted unless necessary, and additional ethical approval was required. All the participants provided written informed consent before participating in the study. Data were processed anonymously. To protect confidentiality, personal information of potential participants and enrolled participants outside the scope of this trial will not be collected, shared or stored before, during or after the trial. The results of this study will be presented at scientific meetings in rehabilitation medicine and in peer-reviewed journals.
Ethics statements
Patient consent for publication
References
Footnotes
BZ and CT contributed equally.
Contributors MF and BZ: designing research studies and acquiring the funding. XZ and CT: involved in the design and improvement of experiments. YYJH and BZ: translated and corrected the manuscript in English. YF and BZ: conducted training and implementation of intervention methods. SF: contributed to the statistical analysis program. QZ: revised the manuscript critically. All authors read and approved the final version of the manuscript. Guarantor is BZ.
Funding This study is funded by the National Natural Science Foundation of China (grant number: 81973973), Construction of an exemplary research ward in Shanghai Shen Kang Center (grant number: SHDC2022CRW010), Shanghai Shen Kang Center Medical Enterprise Integration Innovation Synergy Special (grant number: SHDC2022CRT01) and Chinese Medicine Research Project of Shanghai Health and Health Commission (grant number: 2022QN087), Shanghai Innovative Medical Device Application Demonstration Project 'Application Demonstration of Surface Electromyography' (23SHS05400).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.