Article Text

Abstract
Objectives To evaluate the extent to which organisational factors facilitate or inhibit the implementation of the National Health Service (NHS) carbon reduction strategy within acute hospital settings.
Setting A single acute NHS Trust with four satellite sites which serve more than 2 million patients annually in Central England.
Participants Interviews with a purposive sample of 10 stakeholders, including those who conceptualised the intervention and those who were responsible for its implementation.
Intervention The NHS is a major carbon emitter and therefore developed the ‘NHS carbon reduction strategy (NHSCRS)’ in 2009. NHS organisations are contractually obliged to develop a local carbon reduction strategy known as a Sustainable Development Management Plan (SDMP) which details carbon reduction measures (CRM), as described in the NHSCRS. However, the organisational context within which the SDMP is implemented is likely to determine the extent of its success. We undertook an adapted realist evaluation cycle to develop refined initial programme theories. Documents were analysed using thematic content analysis. Interview data were analysed using thematic analysis.
Results CRM were most likely to be implemented if the Trust Board were sufficiently pressured by staff and reputational fears, and the potential impacts of CRM were perceived to align with wider organisational aims. Differences in implementation of CRM across hospital sites were related to logistical factors, accessibility to regional partners and contractual relationships. There were expected carbon, energy and long-term financial savings, with variability in the effectiveness of some CRM post implementation.
Conclusions Organisational factors, particularly Board leadership and internal implementation pathways, have a significant bearing on whether CRM are implemented or not. However, greater national support and guidance is needed for NHS organisations to effectively reduce their carbon emissions. Further cycles of this evaluation are necessary in multiple case study sites to illuminate the path to a net-zero NHS carbon footprint by 2045.
- health services administration & management
- health policy
- organisational development
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Ethical approval does not permit sharing of raw data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This evaluation fills a critical gap in existing published literature on the implementation of carbon reduction measures within acute hospital settings, how best to mitigate their environmental impact and therefore improve the health of regional populations.
Researchers gathered data using multiple sources such as interviews and documentary analysis, in addition to analysis undertaken with input from methodological experts, which increases the credibility of the findings.
A limitation of this evaluation is that the refined initial programme theory was unable to be tested due to the onset of the COVID-19 pandemic.
Introduction
Climate change, primarily driven by rising greenhouse gas (GHG) emissions, has been declared the ‘the biggest global health threat of the 21st Century’ by an international committee of health and climate change experts.1 Worldwide, healthcare-associated GHG emissions are estimated to account for between 4.4% and 4.6% of total global GHG emissions.2 3 Consequently, climate change presents a twofold challenge for the healthcare sector: (1) to manage the burden of climate change on physical and mental health while (2) mitigating its own GHG emissions.4 5
The UK is widely recognised as an international leader in GHG mitigation, as the first country to legislate ‘carbon reduction’ targets.6 This aims to mitigate the six major GHGs (carbon dioxide, hydrofluorocarbons, methane, nitrous oxide, perfluorocarbons and sulfur hexafluoride) as stated within international climate agreements.7 Since policy documents refer to the mitigation of all six GHGs as ‘carbon reduction,’ ‘carbon’ has been used as an all-encompassing term herein. The UK Climate Change Act (2008) mandates the UK to become carbon neutral by 2050, inline with the Paris climate agreement of 2015.8 This mandates all public sector organisations to match these targets, including the National Health Service (NHS) which contributes 25% of total public sector emissions.9 In 2009, the NHS Sustainability Development Unit (SDU), whose responsibility is to measure, monitor and mitigate NHS carbon emissions, published the world’s first healthcare carbon reduction strategy.10 Known as the NHS carbon reduction strategy (NHSCRS), it details 10 key areas of focus for NHS organisations to reduce their carbon emissions.11 Six of these areas outline carbon reduction measures (CRM) to address the primary sources of NHS carbon emissions, namely, energy, travel, water, waste, procurement and building design.11
The NHSCRS requires NHS organisations to possess a Board-approved Sustainable Development Management Plan (SDMP) to achieve its carbon reduction targets, although only 71% of NHS providers possessed a Board-approved SDMP in 2018.12
In the decade since the NHSCRS release, greater evidence has emerged regarding the potential impacts from implementation of CRM. In 2016, the SDU predicted annual savings of more than £400 million and 1 million tonnes of carbon to achieve a 34% reduction in total NHS carbon emissions (compared with a 2007 baseline) by 2020, if CRM are uniformly implemented across all NHS organisations.13 However, latest NHS data (2017) only indicate an 18.5% carbon reduction since 2007.14 Furthermore, approximately a quarter of NHS Trusts in 2017/2018 missed their interim carbon reduction targets, with only 39% of NHS providers on track to achieve the 2020 interim standard.12 15
SDU data show acute trusts possess the greatest carbon intensity per head of population (210 kg/person), based on services provided, with community, dental and public health services possessing the least (10 kg/person).16 Acute trusts also occupy the largest proportion of NHS estate area (54%), resulting in increased building energy consumption, which forms the second largest proportion of NHS carbon emissions.14 17 Therefore, with acute trusts providing the most carbon intensive services and consuming the most energy, then ensuring CRM are effectively implemented within these settings is most likely to produce the greatest reductions in total NHS carbon emissions.
There is a paucity of published evidence exploring why local carbon reduction strategies and hence CRM remain unimplemented. Isolated studies have indicated the importance of Board level leadership and staff engagement; yet, no studies have assessed stakeholder views in conjunction with implementation processes and outcomes in acute settings.18 19
Aim
We explore the extent to which NHS organisational factors facilitate and/or inhibit the implementation of the NHSCRS in acute hospital settings.
Research questions
To understand the organisational influences which result in the successful implementation (or not) of carbon reduction measures.
To explore the underlying mechanisms and impact of similar carbon reduction measures in different settings.
To explore the consequences of carbon reduction measures on other outcomes, such as finances.
Methods
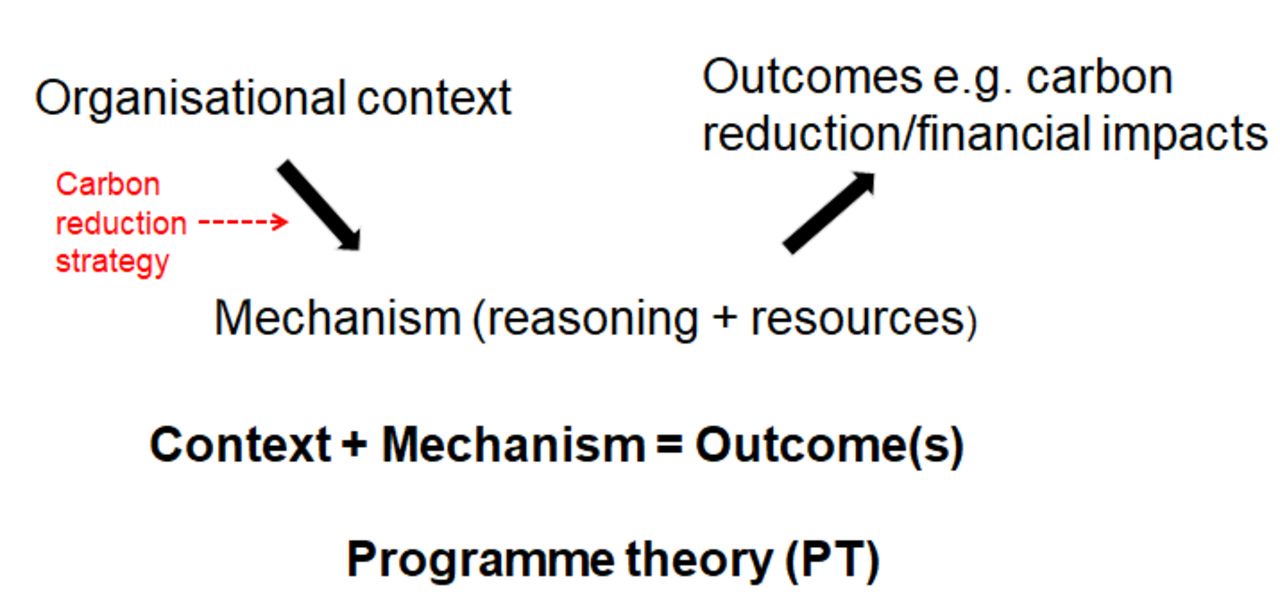
We chose realist methodology for its explicit ability to uncover; the generative processes (mechanisms) which lead to implementation of CRM, the intended and unintended outcomes from implementation of CRM and the role of hospital social environments in enabling implementation to occur (contexts).20 This allowed us to theorise a programme theory in a ‘context-mechanism-outcome (CMO)’ configuration (figure 1).

The ‘intervention’ (the carbon reduction strategy—Sustainable Development Management Plan) is introduced within specific organisational contexts. Consequently, specific ‘mechanisms’ are triggered, thereby leading to outcomes from implementation of carbon reduction measures (adapted from Pawson and Tilley20).
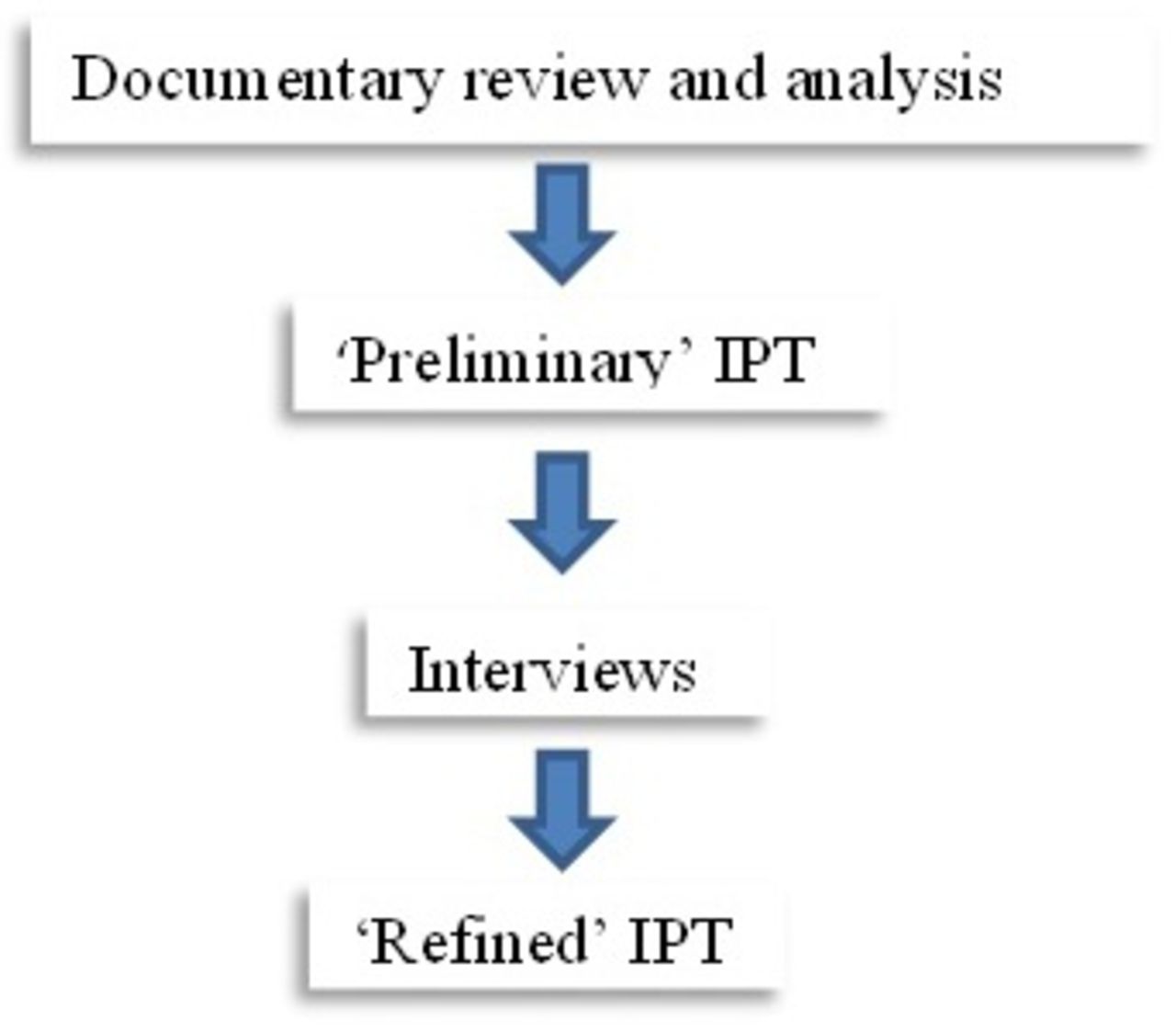
We conducted the evaluation in two stages: (1) theorised a ‘preliminary’ initial programme theory (IPT) following documentary analysis; (2) theorised ‘refined’ IPTs following stakeholder interviews (figure 2). Since the COVID-19 pandemic began mid-way through the study period and restricted access to study participants, we were unable to validate the IPTs. This evaluation is reported in line with the Realist And Meta-narrative Evidence Syntheses: Evolving Standards (RAMESES) II reporting standards.21

Pathway to theorising the initial programme theory (IPT).
Setting
Using a case study approach was deemed appropriate for an in-depth exploration of organisational phenomena.22 Thus, we conducted scoping searches to identify acute NHS Trusts which had implemented an SDMP to select a case study site. Prior literature searching suggested that variation in implementation of CRM is related to geographical, logistical and leadership factors.15 18 19 23 Therefore, we selected one acute NHS Trust with four acute sites (sites A to D) spread across the West Midlands (see table 1). This allowed evaluation of a single implemented strategy (SDMP) and leadership team across multiple geographical and logistical contexts (site A was established more recently vs sites B, C and D). In addition, the Trust began implementation of its SDMP in 2011 which provided sufficient time to analyse outcomes.
Characteristics of the four acute hospital settings
Access to documents and participants was facilitated through a gatekeeper at the acute trust.24 They were involved in both planning and implementing the SDMP, alongside supporting researchers to identify and support data collection with participants.
Data collection
To build the IPT, we purposively searched for documents related to the Trust’s CRM. This was initially informed by the gatekeeper, following which we performed a focused grey literature search within the Trust’s and supporting organisations’ web pages (online supplemental file 1). This yielded the Trust SDMP (n=1), annual reports (n=15), communication articles (n=6) and Board meeting minutes (n=1) (online supplemental file 2). Both qualitative and quantitative data were extracted into a predesigned proforma for easier identification of CMO-related data.
Supplemental material
Supplemental material
To refine the IPT, we conducted one-to-one semistructured interviews to explore stakeholder reasoning and therefore theorise mechanisms for successful implementation. Interview questions were constructed using ‘RAMESES II training materials’ to ensure they were appropriate for capturing relevant data for CMO configurations.25 A topic guide was used to ask questions which began by exploring the participant’s role and function in relation to CRM identified from all documents, followed by participant-specific questions (online supplemental file 3). All interviews were conducted by one member of the research team (SAH), audio-recorded and transcribed verbatim. Although all interviews were planned to be face-to-face, social distancing measures due to COVID-19 required some interviews (n=4) to be completed via telephone. Pseudonyms were given to participants to maintain anonymity.
Supplemental material
Sampling and recruitment of participants
In line with realist evaluation guidance, we initially used purposive sampling to recruit individuals with in-depth knowledge of the Trust’s CRM to refine the IPT (see figure 3).26 We targeted Trust strategists who governed implementation of CRM, since the NHSCRS emphasises the ‘top-down’ nature of implementing CRM.11 Middle managers, who monitored the implementation of CRM across the different hospital sites, were also selected due to their utility in theory refinement.27

Flowchart demonstrating recruitment process.
First, the gatekeeper emailed the target sample (n=11), while the researcher sent a follow-up email attaching a participant information sheet and consent form. Non-responders were sent a reminder at 2 weeks (n=3). To increase the validity of the IPT, we also used snowball sampling to recruit individuals who may have been missed during the initial round of recruitment. This yielded three additional participants. Similar to other realist evaluations, we confirmed our realist hypothesis through ensuring relevance and rigour in the recruitment process.28
Data analysis
Documentary review followed thematic content analysis, as described by Bowen.29 This method was used for its systematic approach to produce CMO configurations. Open and axial codes were applied to documents to form themes within overarching CMO labels.30 31 Quantitative impacts were descriptively coded (online supplemental file 4).
Supplemental material
Interview data were analysed using thematic analysis (online supplemental file 5).32 This was particularly useful to classify the various CMOs to formulate a testable, yet generalisable theory across different typologies of CRM. Both researchers (SAH and MS) coded transcripts using a predetermined coding manual to ensure consistency. Hence, CMO labels were used as overarching themes to which open codes were assigned using NVivo.33 Themes under the CMO labels were then compared and contrasted with the ‘preliminary’ IPT (table 2) to form ‘refined’ IPTs. Interviews and analysis occurred in an iterative manner with weekly meetings between researchers to discuss findings in light of emerging data.
Supplemental material
Preliminary initial programme theory hypothesised from documentary analysis and researcher insights
Throughout the evaluation, we used a reflexive journal to increase transparency of our research conduct and analysis.34 This formed the basis of discussions between the researchers prior to interviews and during data analysis.
Patient and public involvement
Given our focus on strategy and organisational factors, patients and the public were not consulted during study design, data collection or data analysis.
Results
Participant details
We conducted 10 semistructured interviews between February and March 2020. Interviews lasted between 29 and 69 min, with an average duration of 50 min. The sample consisted of both strategists and implementers who had been employed for varying lengths of time (range=1–13 years) (table 3). Strategists included Trust board members who contributed the greatest insight relating to contextual features, while managers gave the most insight into implementation processes.
Participant characteristics
Main findings
Four CMO configurations (CMOcs) became apparent following analysis. Our findings are organised according to these CMOcs.
CMOc 1
When other NHS and non-NHS organisations gain recognition for implementing CRM (C), the Trust Board is more likely to restate its commitment towards the implementation of CRM (O), because of reputational fears and the recognition of prospective positive health impacts from CRM (M).
Policy documents emphasised the reputational pressures to implement CRM. In the short term, this was cited as a consequence of the now redundant (as of 2019) Carbon Reduction Commitment scheme which ranked NHS organisations according to their carbon emissions. Arguably, a more effective and long-term source of reputational pressure was the recognition of neighbouring NHS Trusts implementing a broad range of CRM. This threatened the Trust’s perception as a leader in adopting and implementing novel initiatives:
[Trust name] likes to see itself as a leader, not a follower. Big, big Trust. So let’s not wait till everyone else has done it. (Strategist, board member)
With respect to the moral imperative to reduce carbon emissions (specifically in relation to the ‘threats being posed by climate change’ (2011 SDMP)), the vast majority of documents linked carbon reduction to high-quality patient care. Participants perceived the Trust’s activities as worsening population health through its significant carbon emissions and subsequent direct and indirect health impacts, which could be mitigated through implementation of CRM:
…it would be awful if we’re both simultaneously trying to kind of cure conditions, whilst exacerbating some of the ones that we're seeing with patients. (Strategist, manager)
Annual reports frequently mentioned the occurrence of departmental policy reviews alongside instances of implementing CRM. Thus, reaffirmation of SDMP goals within individual departmental policy is likely to have increased managerial priority to implement CRM:
The Trust’s Procurement policy has been recently reviewed…good procurement practice is critical to carbon reduction. (2013–2014 annual report)
There’s the document [departmental policy] that sends the signal of intent and then there’s the, how do we actually implement this now? (Strategist, senior manager)
CMOc 2
When there is ‘carbon conscious’ and engaged staff who value the implementation of CRM (C), the Trust board is more likely to sustain implementation of a greater range of CRM (O), because the board feels accountable towards its employees (M).
Participants’ spoke at length regarding the increasing level of attention given to carbon reduction by the NHS. Its priority on the national agenda was perceived as ‘pulling its way up the ladder’ (strategist, board member), largely in response to wider public demand. External momentum was perceived as being driven by ‘…things like the Greta [Thunberg] effect and the Australian bushfires’ (operational, estates, 3) resulting in greater priority being given to CRM by both Trust board and staff members alike:
I think that the perception within the Trust is changing and it’s probably because the perception in the NHS, in my view, has escalated quite quickly in the last 12 months. (Operational, estates, 1)
Among Trust board members, this external momentum manifest as CRM being more readily implemented in the face of potential barriers. For instance, there was a relatively small increase in energy costs for the Trust by switching to a renewable energy supplier; yet, there was a perceived general acknowledgement to accept this additional financial burden. As an acute care organisation experiencing a yearly deficit, with no dedicated funding for CRM, this willingness to invest in CRM demonstrated considerable organisational commitment:
So we’ve got a deficit of like 36 million…So it’s huge financial pressures. (Operational, finance)
…there wasn’t enough attention and awareness within the room… That’s a few years ago, that would have been I think the mind-set…but I think we've shifted so that certainly around our executive team it was taken as read, well of course we'll move to green fuel. (Strategist, board member)
There was also a behavioural shift among staff with the introduction of informal carbon reduction ‘champions.’ These were general clinical and non-clinical staff members who were not involved with decision-making or implementation processes; yet, actively concerned about the Trust’s level of carbon emissions. They used staff forums to question the progress of CRM within the Trust, thereby ensuring carbon reduction became, and remained, an organisational priority. Notably, this led to a positive response from the Trust board, with a broader range of CRM being implemented. This ‘bottom-up’ pressure for implementation of CRM was noted to be in stark contrast with the usual ‘top-down’ process of change within the Trust:
…The sustainability work has felt almost the other way around. It’s like the people in the organisation are saying why aren’t we doing more of this? So it’s almost like the board is now, oh God, yeah, we should be doing that. (Strategist, board member)
CMOc 3
When there is increasing healthcare demand resulting in financial pressures (C), implementation of energy and travel-related CRM is dominant (O), because they are perceived to possess the greatest carbon and financial co-benefits (M) and attract the greatest investment from external organisations (M).
Trust leadership stated CRM were often ‘hooked’ onto other agendas. This was perceived to overcome the tensions between a range of organisational priorities, mostly centred on the limited financial resource and, therefore, the need to achieve cost savings. Consequently, CRM aligned with other organisational priorities were more likely to be supported at board level and implemented, since there was greater justification for investment of resources. For example, prior to providing staff transport between hospital sites, purportedly to mitigate carbon emissions, financial and logistical co-benefits were also identified:
Originally it [rationale] was carbon footprint ‘cause transport is a big pollutant. And it reduces costs and parking, ‘cause there’s very little parking on any of the hospital sites. (Operational, transport)
Existing partnerships with organisations were used to accrue additional resource in the form of time, personnel and influence to implement planned CRM, although predominantly travel-related CRM. For example, there was a shared motivation between the Trust and a local academic partner to improve public transport links in the surrounding area. The geographical proximity of these two organisations also appeared to bias the implementation of travel-related CRM towards site A in comparison to other sites:
… they’re [external organisations] the ones that have potentially the biggest impact…those are the ones that potentially are most significant for us to be able to deliver our sustainability strategy. (Strategist, board member)
…although we might have more [employee commuting] data, particularly around travel and transport for [Site A] because of the proximity of the [Academic partner] that have been very good at measuring some of this in recent years. (Strategist, senior manager)
Energy-related CRM (which constituted the majority of all implemented CRM) produced the greatest carbon savings and demonstrated significant long-term financial savings too. The majority were infrastructure-related projects, such as the installation of energy-efficient lighting across all sites (which had a positive impact on staff too) and combined heat and power (CHP) engines at sites B, C and D. Since these required capital expenditure, the financial benefits were limited to lower energy costs in the coming years:
“…the significant lighting investment-it’s created a better environment for people that are working in there…the amount of light in the area was quite dim…the feedback we had was generally very positive. Ultimately, um, the balance sheet is helped by the investments ‘cos each year we get a cost improvement program where we have to make savings. (Operational, estates, 2)
CMOc 4
When there is logistical or contractual obstacles to implementing CRM (C), the range of CRM implemented across hospital sites is limited (O), because there is no dedicated sustainability team with the personnel and time needed to liaise with all relevant stakeholders to successfully implement a wide range of CRM (M).
CRM were implemented through multiple streams (estates and facilities, transport and procurement departments), such that departments were often required to engage with internal and external stakeholders to achieve similar aims. The estates department engaged with external contractors for infrastructure projects and also internal staff to support energy saving campaigns. Consequently, participants frequently cited the need for specific individuals to coordinate the various streams of implementation:
We don’t have a dedicated sustainability team. We have people who are involved and that’s why we can chip away at this for so long. I'll be very clear-we can carry on doing some stuff, but probably can’t do it as comprehensively. (Strategist, senior manager)
To implement energy efficiency infrastructure projects, new contractual relationships were needed for both technical and construction expertise. Challenges for the Trust emerged in gaining buy-in from existing contractual relationships, particularly with site A’s private finance initiative (PFI) provider (To fund large public infrastructure projects, such as hospital buildings, the private sector is often contracted to provide the initial capital cost of projects, and in many cases to also provide continuing management and funding of these projects. The private company who performs these functions is known as the Private Finance Initiative (PFI) provider. Contracts typically last between 25 and 30 years) and Trust suppliers. Since the PFI provider owns a large proportion of site A’s estate, CRM involving infrastructure and utility changes required their approval beforehand. Hence, most CRM implemented at site A were procurement and travel-related, in contrast with the other three sites in which energy-saving infrastructural changes requiring capital expenditure were more abundant:
…we just have less control over what we can change here [Site A] as a result of that [PFI contract]. We have more control over our other sites. (Strategist, senior manager)
The geographical location of hospital sites appeared to impede the effectiveness of travel-related CRM. The numbers of staff cycling or using public transport at site B remained ‘fairly static’ (operational, transport) compared with the increase in use of public transportation/cycling across the other three sites. It transpired the location of site B was such that it made staff feel unsafe, perhaps due to a perception of increased crime within the vicinity. Thus, although bus and cycle shelters were installed, their usage was limited:
…some staff have said “in the winter when it’s dark, I feel a bit vulnerable walking off-site ‘cause we don’t have any security around, particularly if you’re working late”… that could be a barrier to them cycling… staff wouldn’t feel as safe cycling to [Site B] as they were cycling to [Site A]. (Operational, human resources)
Of all the outcomes described, the most significant was the risk of CHP engines emitting greater carbon than the electricity supplied by the National Grid, potentially jeopardising the accrued carbon savings at sites B, C and D. The ability to overcome this was limited by the long-term contract with the external contractor, which could only be revisited once the contract expired:
…as the grid decarbonises, the idea of CHP instead of saving carbon, actually emitting more carbon because the emissions factor of gas aren’t expected to change vs electricity factors which will go down. (Operational, estates, 1)
Discussion
Summary of findings
We conducted an adapted realist evaluation of a single acute NHS Trust’s carbon reduction strategy (SDMP), focusing on the organisational factors which affected its implementation. We found these to be a combination of factors both internal and external to the Trust. Our findings reveal common mechanisms affecting all sites; but, also variation in type and range of implemented CRM across sites. We produced ‘refined’ IPTs, suitable for testing in further evaluation cycles (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Refined initial programme theories (IPTs)—the main differences between the preliminary IPT and refined IPT are in red. Themes are in bold type. CRM, carbon reduction measures.
Among the CMOcs we identified, internal staff pressure and accountability was crucial for implementation of CRM. This was inevitably linked to the increasingly favourable wider public opinion towards healthcare carbon reduction efforts which diffused into the workplace, even among board members. Owing to the diversity of CRM, differences in implementation of CRM across different hospital settings were dependent on the availability of regional stakeholders, logistical factors and, in one case, the PFI provider.
However, we also discovered a mechanism common to all implementation processes; CRM which were perceived to possess greater co-benefits were more likely to be implemented. This mechanism was ‘triggered’ by the limited resources (financial and personnel) available. Consequently, implementation of all six types of CRM detailed within the NHSCRS was not evident; with the majority of implemented CRM belonging to energy, travel and procurement, that is, those mostly associated with external funding and/or partner organisations. Since CRM were implemented through individual departments (eg, travel-related CRM through the transport department and energy-related CRM through the estates department), departmental managers were responsible for the majority of downstream implementation processes. This was deemed to limit the scope of CRM implementation as there was no dedicated ‘implementation’ team.
There was little evaluation of the outcomes from implementation, beyond the expected carbon, financial and energy savings. By definition, all CRM are intended to produce carbon savings; however, we revealed two possible reasons this aim may not be achieved post implementation. First, the effectiveness of a variety of travel-related CRM (eg, bus and cycle shelters) was confounded by staff security fears, particularly at site B. Therefore, greater stakeholder engagement prior to, or in conjunction with, implementation of CRM is necessary. Second, and perhaps more significantly, we discovered CHP engines are projected to no longer be viable for carbon reduction purposes. Our findings also demonstrate that the typology of implemented CRM affects different subgroups differently. For example, general hospital staff were not directly affected through many energy initiatives, for example, CHP engines; yet, energy-efficient lighting reportedly had positive staff impacts.
Relevance of findings and implications
Our findings showed reputational drivers were important sources of pressure for board members to implement the Trust SDMP, concurring with views expressed by NHS leaders elsewhere.19 Nationally, NHS staff support for CRM has increased over the years, yet the manner in which this has manifested within NHS organisations has been unclear.35 In contrast with other NHS organisations in which implementers (eg, managers) were most vocal on carbon reduction, we found staff external to implementation processes championing implementation of CRM.36 This discrepancy could partly be explained by the presence of dedicated sustainability teams implementing CRM elsewhere. Nevertheless, the necessity for internal staff pressure to implement CRM signalled the absence of strong Board leadership.
Poorly coordinated implementation of CRM led to consensus among participants for dedicated ‘sustainability’ job roles. NHS leaders have previously cited uncertainty regarding the effectiveness of dedicated roles, compared with more diffuse implementation pathways.18 Evidence highlights that dedicated job roles in and of themselves do not aid implementation of CRM, unless there is adequate buy-in from senior leadership, underscoring the necessity for Board level support and leadership for successful implementation of CRM.37–39 We showed Board level support can be gained by promoting alignment between CRM and other organisation-specific priorities.
The impact of shifts in public opinion towards favouring carbon mitigation featured heavily within our findings.40 With increasing public pressure on implementing carbon reduction policy, Naylor and Appleby suggested this early impetus for carbon reduction may have adversely affected CRM implementation within hospitals.23 NHS managers opted to implement CRM with ‘quick wins’; those which effectively reduced carbon emissions and demonstrated the greatest financial savings within the shortest period of time, such as installing energy-efficient lighting. This ‘short-termism’ limited the range and typology of implemented CRM, preventing implementation of larger infrastructure or travel-based CRM, and hence total carbon reduction potential.23 Our findings suggest NHS managers and board members are now more willing to commit to long-term CRM projects, although these require overcoming other regional and logistical barriers.
Regional support for NHS organisations to implement CRM is also expected to increase, with 74% of local authorities declaring a ‘climate emergency’—a statement of intent to achieve net-zero carbon emissions prior to 2050.41 Since hospitals and acute care comprise the majority of the £13 billion NHS PFI schemes, it is possible many NHS organisations are avoiding infrastructure-based CRM.42 The NHSCRS briefly mentions PFI providers stating they ‘must be able to demonstrate long term low carbon performance,’ suggesting this refers to early dialogue with PFI providers, as opposed to negotiating during implementation.11 Our findings highlight that NHS organisations should consider the financial implications associated with implementing infrastructure-based CRM in the context of PFI constraints. Furthermore, although the NHS intends to achieve net-zero emissions for ‘direct’ emissions, for example, through reducing building energy usage, by 2040, this is a difficult task without the buy-in of PFI providers, whom are often responsible for hospital infrastructure. As such, we recommend the national policy makers to engage with PFI providers to proactively implement CRM and reduce emissions in line with national targets.
The pace of decarbonisation within a number of different sectors, particularly the energy sector, has impacted the effectiveness of technological energy-related CRM. CHP engines were touted by the SDU as producing the greatest carbon and financial savings for acute hospitals, and case studies have attested to their significant impacts.18 43 Yet, from 2021, CHP engines will emit greater carbon emissions than the electricity supplied by the national grid, nullifying the original purpose for which CHP engines were installed.13 On-site renewable energy sources have been proposed as ensuring longer-term carbon savings.44 This is limited by the availability of appropriate on-site renewable power generation technology capable of meeting the 24/7 energy demands of acute hospital settings. How NHS organisations can, or should, introduce renewable energy remains in question with many currently constrained by long-term energy contracts before alternative arrangements can be considered.
Strengths, limitations and future directions
To our knowledge, this is the first study exploring organisational factors that are responsible for the implementation of CRM in a UK healthcare setting, from strategy to implementation. This evaluation fills a gap by exploring why local carbon reduction strategies (SDMPs) have achieved differential outcomes across different hospital settings, and the extent intra-organisational and inter-organisational factors are responsible. Using documents and interview data provided a strong methodological basis to this evaluation, as did bilateral transcript analysis. Although we have elucidated specific CMOcs which can be tested, it is likely there are a greater range of proximal/intermediate outcomes we have not discovered on the path to implementation of CRM. As such, we recommend further evaluation cycles to explore these with relevant stakeholders, especially since we were unable to access external stakeholders as a result of the COVID-19 pandemic curtailing our data collection. Likewise, further economic evaluation and statistical analysis of quantitative impacts will elucidate which CRM provide the greatest carbon and financial savings in practice.
Conclusions
This novel evaluation adapted realist methodology to provide insight into a range of organisational factors, aligning governance processes and stakeholder views with actual outcomes to truly understand the factors which may facilitate or inhibit implementation of CRM. This study has provided refined IPTs detailing provisional action which can be taken to achieve wide scale and effective implementation of CRM. Further cycles of this evaluation in multiple case study sites is required to illuminate the path to a net-zero carbon NHS by 2045, thereby improving the health of both regional and national populations.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Ethical approval does not permit sharing of raw data.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the University of Birmingham Internal Research Ethics Committee on 7 January 2020 (Reference: IREC2019/1518061). All participants volunteered to take part and provided written consent. Data were anonymised with respect to individuals and institutions.
Acknowledgments
The authors wish to thank the NHS Trust and in particular the gatekeeper for expressing interest in the study and facilitating it. Many thanks also to the participants who volunteered their time for interviews, especially during the COVID-19 pandemic.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SAH and MS conceived the study design. SAH designed study materials and gained ethical approval. Both authors contributed to data analysis. SAH wrote the first draft of the manuscript with input from MS. Both authors approved the final manuscript.
Funding MS is funded by the National Institute for Health Research, Health Services and Delivery Research programme (HSDR 16/138/31 – Birmingham, RAND and Cambridge Evaluation Centre).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.