Primary care management of patients after weight loss surgery
BMJ 2016; 352 doi: https://doi.org/10.1136/bmj.i945 (Published 10 March 2016) Cite this as: BMJ 2016;352:i945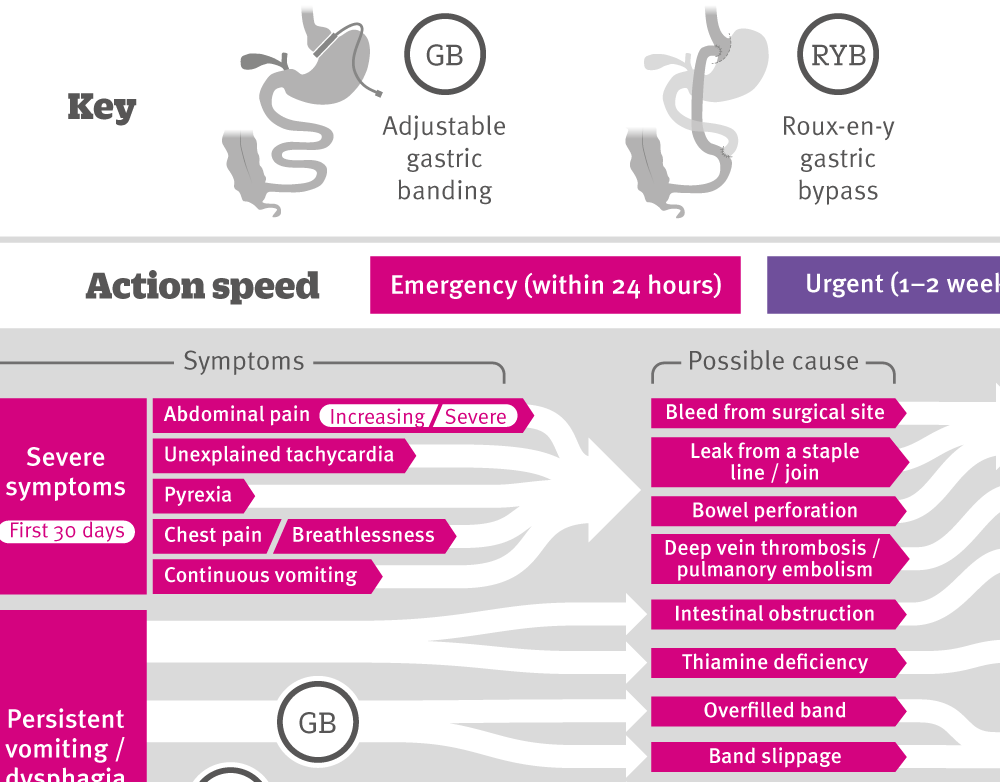
[Infographic] Assessing and referring complications following bariatric surgery
Explaining symptoms that warrant referral to bariatric and/or surgical teams, including possible causes, referral speed and recommended actions.

Chinese translation
该文章的中文翻译

- Michael Moore, professor of primary care research1,
- James Hopkins, senior bariatric fellow and honorary research fellow2 3,
- Patrick Wainwright, specialist registrar in chemical pathology and metabolic medicine4
- 1Primary Care and Population Sciences, Faculty of Medicine, University of Southampton, Southampton, UK
- 2Musgrove Park Hospital, Taunton, UK
- 3University of Bristol, Bristol, UK
- 4Clinical Biochemistry, University Hospital Southampton, Southampton, SO16 6YD, UK
- Correspondence to: M Moore mvm198{at}soton.ac.uk
What you need to know
In the first 30 days after bariatric surgery, symptoms such as increasing or severe abdominal pain, unexplained tachycardia, pyrexia, chest pain or breathlessness, or continuous vomiting warrant emergency referral
Continue long term monitoring of cardiovascular risk and comorbidities associated with obesity, such as type 2 diabetes; reduce treatment for these as appropriate
All patients need lifelong supplementation with vitamin and mineral supplements to prevent serious nutritional complications
Bariatric surgery is the most effective treatment for sustained weight loss in people with complex obesity,1 2 and reports from large UK and international registries highlight its overall safety.3 4 The overall mortality of 0.07% and composite complication rate of less than 4% for gastric bypass are similar to those for laparoscopic cholecystectomy.4 After surgery, short hospital stays are the norm (median one day for gastric band and two days for a sleeve gastrectomy or gastric bypass).2 General practitioners thus need to recognise early, as well as late, postoperative complications, monitor long term nutrition, and provide support. General practitioners may also need to assess patients who have had bariatric surgery abroad (sometimes with non-standard procedures), without any follow-up planned. Useful resources for patients include BOSPA (http://www.bospauk.org) and WLSinfo (http://www.wlsinfo.org.uk).
The operations
Box 1 describes the three most common procedures performed in the United Kingdom. More than 95% are done laparoscopically.3 5
Box 1: Most common bariatric surgery procedures in UK (fig 1⇓)
Laparoscopic adjustable gastric banding
An adjustable band is placed around the top of the stomach, forming a small gastric pouch above it. The band is adjusted by injecting saline into a port positioned under the skin to achieve the sensation of fullness after a small amount of food.
Roux-en-Y gastric bypass
The most common operation for weight loss in the UK NHS (60%), involving creation of a small gastric pouch by stapling. A classical Roux-en-Y reconstruction is then fashioned with …
Log in
Log in using your username and password
Log in through your institution
Subscribe from £184 *
Subscribe and get access to all BMJ articles, and much more.
* For online subscription
Access this article for 1 day for:
£50 / $60/ €56 (excludes VAT)
You can download a PDF version for your personal record.