Article Text

Abstract
Background Chronic non-cancer pain (CNCP) treatment’s primary goal is to maintain physical and mental functioning while improving quality of life. Opioid use in CNCP patients has increased in recent years, and non-pharmacological interventions such as music listening have been proposed to counter it. Unlike other auditive stimuli, music can activate emotional-regulating and reward-regulating circuits, making it a potential tool to modulate attentional processes and regulate mood. This study’s primary objective is to provide the first evidence on the distinct (separate) effects of music listening as a coadjuvant maintenance analgesic treatment in CNCP patients undergoing opioid analgesia.
Methods and analysis This will be a single-centre, phase II, open-label, parallel-group, proof-of-concept randomised clinical trial with CNCP patients under a minimum 4-week regular opioid treatment. We plan to include 70 consecutive patients, which will be randomised (1:1) to either the experimental group (active music listening) or the control group (active audiobooks listening). During 28 days, both groups will listen daily (for at least 30 min and up to 1 hour) to preset playlists tailored to individual preferences.
Pain intensity scores at each visit, the changes (differences) from baseline and the proportions of responders according to various definitions based on pain intensity differences will be described and compared between study arms. We will apply longitudinal data assessment methods (mixed generalised linear models) taking the patient as a cluster to assess and compare the endpoints’ evolution. We will also use the mediation analysis framework to adjust for the effects of additional therapeutic measures and obtain estimates of effect with a causal interpretation.
Ethics and dissemination The study protocol has been reviewed, and ethics approval has been obtained from the Bellvitge University Hospital Institutional Review Board, L’Hospitalet de Llobregat, Barcelona, Spain. The results from this study will be actively disseminated through manuscript publications and conference presentations.
Trial registration number NCT05726266.
- Chronic Pain
- Pain management
- Quality of Life
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This is a proof-of-concept, open-label, randomised clinical trial assessing the effects of music listening (a non-pharmacological approach) on pain perception, anxiety, depression and opioid requirements.
To separate the effect of music listening from that of other interventions, and in particular opioid therapy, we will use mediation analysis implemented through two rounds of the recursive g-formula.
To account for potential interactions between music listening and opioid therapy, we will use a four-way effect decomposition.
The open-label design, relatively small sample size, and a study population restricted to patients attending a tertiary medical centre may limit our findings.
Background
Chronic pain is a common, multifaceted and distressing issue supposing a significant societal and individual burden.1 Its management can be challenging, with approximately 20% of patients requiring opioid treatment.2 Chronic pain heavily burdens healthcare and welfare systems due to high demand and economic aid requirements, thus making it an important health and social care challenge that should not be overlooked.3–5
Chronic non-cancer pain (CNCP), defined as pain lasting beyond the time of tissue healing or for over 3 months,6 has a marked impact on quality of life (QoL) and psychological well-being, imposing daily life limitations and restricting community participation. The primary goal of CNCP treatment is maintaining physical and mental functionality while improving QoL. Although pharmacotherapy plays a primary role, a multimodal approach may be needed, including, besides medication, psychological therapy, active physiotherapy, occupational and movement therapies, or percutaneous electrostimulation, among others.7
Regarding pharmacotherapy, combining analgesic drugs, is often required to achieve pharmacological synergy while reducing side effects.8 Opioids are the most potent analgesics and remain the go-to medication for chronic pain patients, but they may cause significant side effects and tolerance.9 Moreover, opioid use in high-income countries has increased in recent years,10–12 and a major part of the consumption is due to CNCP.10 As a response, different behavioural therapies have been proposed to potentiate the analgesic effects of opioids and, consequently, reduce the required doses. One of these behavioural therapies consists of listening to music therapeutically—as a cognitive tool to modulate attentional processes and regulate mood.
Listening to music is one of the most common leisure activities. Its therapeutic use lies in its emotional-regulatory and mood-regulatory properties.13 Cognitive-level music processing requires perceiving basic (frequency, duration, volume) and high-order (harmony, intervals, rhythm) acoustic characteristics, attentional processes, recruiting and working and episodic memory.14–19 Unlike other auditive stimuli, music listening can activate emotional-regulating and reward-regulating circuits, making it a potentially useful tool in clinical settings. Its exact mechanism of action in the central nervous system remains not fully understood. Still, music listening seems to act on different brain areas (eg, nucleus accumbens, amygdala, hippocampus),20–22 promoting neurotransmitter release (eg, dopamine, endogenous opioid peptides) in key regions of the motivation and reward systems.23 Some clinical studies have demonstrated that music can improve pain perception, anxiety, depression and reduce opioid requirements in postsurgical chronic pain patients.24 25 Markedly, music listening has greater effects on pain when listened before the onset of the day’s most severe pain intensity—by preventing pain-related anxiety and depression that often precedes or follows pain onset, respectively.24
Remarkably, opioid consumption patterns differ between men and women. Higher rates of prescription opioid use among women have been reported,26 27 as well as a higher risk of opioid use disorder and of experiencing a greater disease burden than men.28 A 2015 systematic review reported that women are more likely to adopt maladaptive pain coping strategies—increasing the risk of chronification.29 Furthermore, factors such as higher incidences of anxiety and/or depression (both also comorbidities associated with chronic pain) and social factors (eg, economic dependence) may impact the consumption of drugs with the potential for abuse.30–32 Thus, it is paramount to adopt a sex perspective when addressing this issue, considering sex as a biological variable to improve health interventions and increase the scientific rigour and the results’ generalisability.
This manuscript describes the study protocol of a proof-of-concept randomised clinical trial that aims to assess the effect and safety of music listening as a coadjuvant to the analgesic opioid-based treatment for CNCP patients.
Explanation for the choice of comparators
Patients randomised to the control group will actively listen to audiobooks. Listening to audiobooks is a widely accepted control intervention used in studies assessing the benefits of listening to music since it is also based on information-presenting auditive stimuli.33 34
Although some authors have adopted standard care without any auditive stimuli as control,25 the new framework for developing and evaluating complex interventions by the Medical Research Council recommends considering the experimental intervention’s main components when choosing the control group.35 Thus, control interventions should have similar characteristics to the experimental ones, except for those hypothesised as elements responsible for the benefits. In this case, both music and audiobooks require an active effort in terms of auditive stimuli, but only music has the intrinsic ability to elicit emotions and regulate mood.
Hypothesis and objectives
Our working hypothesis is that music-listening (as a coadjuvant to regular opioid analgesic treatment) reduces pain intensity in CNCP patients. Consequently, daily opioid consumption and the likelihood of developing tolerance, dependence and opioid-related adverse events (AEs) shall be reduced, whereas emotional well-being and QoL shall improve.
Our primary objective is to provide evidence on the distinct (separate) effect of listening to music as a coadjuvant maintenance analgesic treatment in CNCP patients undergoing opioid analgesia.
Our secondary objectives are, in CNCP patients undergoing opioid analgesia:
To assess the effect of listening to music on anxiety, depression and mood.
To assess the effect of listening to music on QoL.
To assess the effect of listening to music on the development of tolerance, dependence and risk of addiction to opioid-based analgesic treatment.
To estimate which clinical, sociodemographic and baseline analgesic treatment variables predict a greater analgesic response to listening to music as a coadjuvant maintenance analgesic treatment.
To assess the safety of listening to music as a coadjuvant maintenance analgesic treatment.
Methods/design
Study design
This study will consist of a single-centre, phase II, open-label, parallel-group, proof-of-concept randomised clinical trial. Individual participant duration will last approximately 16 weeks. The study is planned to start in May 2023, and we expect it to end in May 2025.
Study settings and population
This clinical trial will be carried out at a tertiary medical centre with a service area covering over two million people in the Barcelona south metropolitan area. The study population will consist of CNCP patients under regular opioid treatment for at least 4 weeks.
Eligibility criteria
Patients meeting all inclusion criteria and none of the exclusion criteria will be eligible for this trial. Eligibility assessment will be performed by the pain clinic physician during study visit 1 and will be reassessed during study visit 2, before the randomisation (see the Participant timeline section).
Inclusion criteria:
Patients ≥18 years of age, of both sexes.
Diagnosed with CNCP.
Under regular (maintenance) opioid treatment for at least 4 weeks.
Those who sign the written informed consent.
Exclusion criteria:
Pregnant or lactating women.
History of an organic brain disorder.
History of substance abuse/dependence.
History of psychotic disorder, bipolar disorder and/or intellectual disability.
Patients with a high risk of opioid addiction.
Patients deemed non-cooperative by the pain clinic physician or therapists (ie, likely to not adhere to treatment).
Eligible patients chronologically visited in our tertiary medical centre pain clinic by a study team investigator will be invited to participate in the study until reaching a sample size of 70 patients (see the Sample size section).
Interventions
Consecutive patients will be randomised (1:1) to one of the two study groups: experimental (music-listening) or control (audiobook-listening). Patients will actively listen to either music (experimental group) or audiobooks (control group) for at least 30 min (up to 1 hour) a day for 28 days. The instruction of listening to music or audiobooks for at least 30 min and up to 1 hour is given to ensure similar fixed hours of exposure to music or audiobooks between participants and control for intervention intensity.
Once the randomisation is carried out, an occupational therapist experienced in music-based rehabilitation will conduct an interview focused on each participant’s randomised intervention.
For patients in the music group, the interview will be based on the Music Assessment Tool to assess music preference standardly.36 This evaluation includes sociodemographic questions that influence music preference, if the patient likes to listen to music, whether they play an instrument and their level of musicianship, queries about reasons to listen to music, questions regarding preferred music genres, groups and artists, instruments and sounds, and questions about the music, artists and instruments the patient dislikes. Additionally, two open-ended questions about cultural considerations for music selection and any other information the patient may wish to provide will be asked. The information gathered during this interview will be used to create a playlist of favourite and preferred songs, which will be developed in collaboration with the patient. A music therapist will later supervise the interview responses and the playlist, which will be created on an online music-player platform using individual accounts for each participant. The occupational therapist will assist patients in installing the music-player app on their mobile phones if they do not already have it and provide instructions on its use. Patients will be able to modify their playlists during the intervention, either by adding or deleting soundtracks.
For patients in the audiobook group, the occupational therapist will follow a similar procedure used in the music group, but the interview will focus on the patient’s favourite type of reading. This evaluation will include sociodemographic questions influencing reading preferences, whether the patient likes to read, the number of books read during the previous year, questions about reasons to read and preferred literature genres, authors, books on wishlist, and disliked genres, books and authors. Furthermore, two open-ended questions will be asked about cultural considerations for audiobook selection and any other information the patient may wish to provide. The information gathered during this interview will be used to create a playlist of favourite and preferred audiobooks on an online audiobooks platform, which will be developed in collaboration with the patient. The selection will be created using individual accounts for each participant. The occupational therapist will assist patients in installing the app on their mobile phones if they do not already have it and provide instructions on its use.
In both groups, the intervention will be self-administered using participants’ own mobile phones and headphones. Patients will be instructed to find a quiet moment and place at home where they can be alone and listen to the preset music or book playlist continuously and keenly, focusing on the listening experience without engaging in simultaneous activities or seeking companionship. Notably, we will ask them to listen to it before 20:00 hours since they will also need to answer pain intensity and mood status questionnaires at the end of the day; however, we will conduct an interview to get to know their daily routines and agree on the best moment during the day for them to listen to their randomised intervention.
Throughout the intervention, the occupational therapist will monitor patients, their daily evaluation responses, and treatment adherence virtually (see the Outcomes section). We recognise that patients might listen to music or audiobooks anytime during the day (eg, while cooking or driving); thus, we will inquire them daily whether they have engaged in these activities outside of the designated intervention period. Additionally, weekly phone calls will be made to address any questions or issues. Adjustments to the music playlist or audiobooks will be performed during these phone calls based on individual preferences.
Criteria for discontinuing or modifying allocated interventions
Participation in the study is voluntary. Patients may withdraw their consent to participate at any time without giving any justification; no penalty whatsoever shall affect the healthcare they are entitled to receive.
On the other hand, the investigator may discontinue any participant that:
Continually fails to comply with the study procedures (ie, repeated protocol violations).
Is lost to follow-up.
Becomes pregnant during the trial.
Is deemed (according to the investigators’ clinical judgement) to present an unacceptable benefit–risk ratio related to any study procedure.
CNCP-related comorbidities will not be considered criteria for discontinuation. The investigators will register the reason for discontinuation/withdrawal on the source document, patients’ individual medical records, and the specific electronic case report form (eCRF) section.
If the reason for discontinuation is a serious AE (SAE), we will follow the participants until resolution or stabilisation. Obtaining the follow-up data of the patients withdrawn because of SAEs is mandatory. In any case, we will make every effort to carry out the security and monitoring procedures specified in the protocol.
All patients withdrawn from the study will complete the end-of-study (EoS) visit. They will be able to continue the study treatment (if they wish to), and analgesic treatment will be prescribed according to standard clinical practice.
Strategies to improve adherence to interventions
Listening to music is a self-administered therapy that can be performed in almost any quiet environment. Participants who do not own speakers or headphones will be provided with such for the purpose of this trial.
A mobile app has been designed within the framework of this project and allows patients to register their pain intensity and mood status information daily; it also records whether the intervention is performed or not.
Patients will receive automated notifications through the app if they have missed a daily session. The study occupational therapist will be able to monitor treatment adherence and questionnaire fulfilment electronically. Moreover, we will perform phone calls to assess difficulties with the app and encourage patients to keep all study-related procedures.
Relevant concomitant care permitted or prohibited during the trial
No concomitant care is prohibited during the trial.
Outcomes
The primary and secondary outcome measures, as well as their justifications, are summarised in table 1. Importantly, chronic pain is a multidimensional condition; thus, we are facing a clinical trial where two or more primary variables are needed to describe clinically relevant treatment benefits, and no formal adjustment is necessary.37 38
Primary and secondary outcome measures
At the beginning of the study, participants will receive a diary to complete a daily evaluation. Each evening, participants are asked to report the maximum pain intensity experienced during the day, the specific time they experienced it, any use of rescue medication, their mood and energy levels, and whether pain interfered with their daily activities. During the intervention phase, participants will continue to complete the daily evaluation, but this time using an ad-hoc designed app. The app will present the evaluation questions in a user-friendly form-based format. The app will also include queries about the time spent listening to music or audiobooks. Patients will also be asked whether they listened to music or audiobooks during times other than the designated intervention period, when they engaged in this activity, and how long they spent doing so.
Participant timeline
Participant timeline is summarised in table 2. For a detailed description of each visit’s procedures, please refer to the section Plans for assessment and collection of outcomes.
Participant timeline
Sample size
Given the proof-of-concept and exploratory nature of the present clinical trial, the sample size is not based on ensuring statistical power but vice versa, the statistical power yielded by the feasible sample size was prechecked to ensure relevance. We will include a total of 70 consecutive eligible patients; 35 will be randomised to each of the groups. With such sample size, the statistical power to detect a minimal clinically important difference in pain intensity of 2 cm in the 10 cm Visual Analogue Scale (VAS) between study arms in a repeated measures design,39 with at least three summary measurements per patient and a moderate autocorrelation of 0.3, will be 81.7% at a significance level of 5% when the SD is 4 cm.
After performing some simulations, we have verified that if there were differences in pain intensity of such magnitude between the study groups, we would come out with significant total and, probably, direct effects of music listening with a causal interpretation. However, if the differences only concerned the opioid doses but not pain intensities, the planned sample size would be insufficient to declare the indirect effects as significant. In such a case, nevertheless, we could almost certainly declare a benefit in terms of significant reductions of opioid requirements, which would have also a causal interpretation because the primary intervention (music or audiobook listening) is actually randomised.
Recruitment
Recruitment will be performed in visit 1, which may include more than 1 day. Potential participants will be visited in the pain clinic by a physician and a psychologist from the study team. The pain clinic physician will confirm the CNCP diagnosis and that the patient meets all the inclusion criteria and none of the exclusion criteria. Patients will receive the ‘patient information sheet’; the investigator will explain the study in detail, inform that participation is voluntary, and answer any doubts that may arise. Those who decide to participate will be asked to sign the informed consent form, and no study-related procedure will be performed prior to signing this form.
Sequence generation, concealment and blinding
After ensuring the participant still meets all the eligibility criteria, the pain clinic physician (during visit 2) will introduce the participant’s data corresponding to visit 2 in the eCRF (see the Data management section). The eCRF automatically allocates the participant to one of the study groups. Importantly, although the psychologist will not be aware of the patients’ randomised group, the pain clinic physician and the occupational therapists will become aware of it, given the open-label design.
Blinding is unfeasible for cognitive behavioural therapies and will not be performed; however, the investigators performing the evaluations will not be aware (blinded) of the assigned interventions. The allocation will follow a computer-generated sequence of random permuted blocks of size 4 or 6. Numbered codes will be assigned to included patients in an ascending sequential order. The randomisation list will be stored in our medical centre clinical research support unit.
Plans for assessment and collection of outcomes
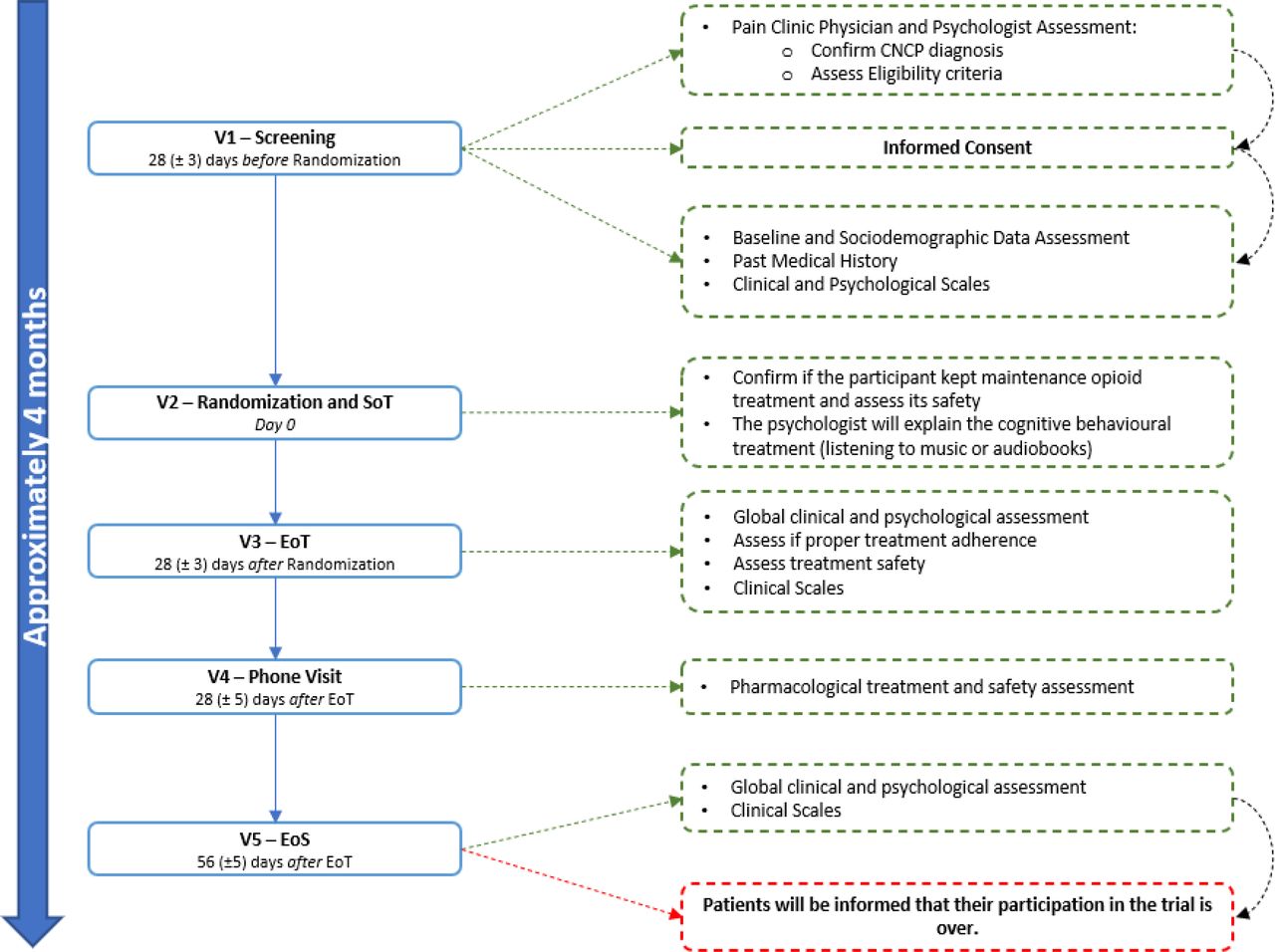
Figure 1 summarises the study scheme. The screening visit (visit 1) will be performed 28 (±3) days before starting the treatment. Recruited patients (see the Recruitment section) will undergo fit-for-purpose clinical evaluation during visit 1. Additionally, we will gather their baseline and sociodemographic characteristics and clinical and laboratory data from their medical records. They will be asked to answer all the clinical scales and questionnaires related to the study objectives (see table 1), such as: (1) the VAS,40 (2) the McGill Pain Questionnaire,41 42 (3) the Hospital Anxiety and Depression Scale, (4) the Short-Form 36 Health Survey (SF-36),43 (5) the EuroQoL 5 Dimensions 5 Levels Questionnaire (EQ-5D-5L),44 (6) the Profile of Mood States (POMS),45 (7) the Opioid Risk Tool46 and (8) the Revised Screener and Opioid Assessment for Patients with Pain.47

Study scheme. CNCP, chronic non-cancer pain; EoS, end of study; EoT, end of treatment; SoT, start of treatment; V, visit.
Psychological scales and questionnaires will also be administered during this visit. They will allow for describing and controlling individual differences that may act as confounders, such as: (1) sensitivity to music reward (pleasure derived from musical experiences), to be assessed with the Barcelona Music Reward Questionnaire,48 (2) perceived social support, to be evaluated by the Medical Outcomes Study-Social Support Survey,49 (3) presence and impact of traumatic events, to be assessed by the self-applied Life Events Inventory,50 (4) self-esteem, to be measured by the Rosenberg Self-Esteem Scale,51 and cognition, to be assessed by the Montreal Cognitive Assessment.52
Participants will be handed the ‘participant diary’ and asked to register the current pain intensity, the maximum pain intensity in the last 24 hours, and the mean pain intensity in the last 24 hours. They will be asked to do so every day during 4 weeks and after 20:00 hours.
Visit 2 will be the randomisation and start-of-treatment (SoT) visit (day 0). The pain clinic physician will confirm that the participant has been on opioid maintenance analgesia since visit 1 and review the patient’s diary. The safety of opioid treatment will be assessed by directly questioning the participant about common AE. Additionally, the eligibility criteria will be reassessed. Only after confirming that the participants still meet all the inclusion criteria and none of the exclusion criteria will they be randomised. The study occupational therapist will explain the cognitive behavioural therapy procedures and will reassess all the emotional outcomes mentioned in table 2. The control and experimental interventions will be performed as described in the Interventions section.
Visit 3 (end-of-treatment visit, EoT) will be performed 28 (±3) days after the SoT visit by the pain clinic physician and psychologist. They will perform a global clinical assessment, confirm that the participant performed all study-related procedures properly, and perform a safety assessment. Patients will be asked to answer the Patient Global Impression of Change scale.53 Opioid treatment will be adjusted, if required, and participants will be allowed to keep the music/audiobook therapy sessions if they wish to do so.
Visit 4 will consist of a phone call visit and will be performed 28 (±5) days after the EoT visit to assess pharmacological treatment safety.
Visit 5 will be the EoS visit and will be performed 56 (±5) days after the EoT; the pain clinic physician and psychologist will perform a final clinical assessment and will inform the participants that their participation is concluded.
Plans to promote participant retention and complete follow-up
An ad hoc ‘app’ has been created for this study. It will send patients notifications to ensure treatment adherence (listening to music or audiobooks), allow patients to insert study-related data (eg, maximum pain intensity in the last 24 hours, current pain intensity, mood state, safety), and collect daily information on breakthrough pain and need for rescue analgesia.
Study treatments will be self-administered through the electronic devices the participant has available; we will provide speakers or headphones for those who do not have them. Additionally, we will perform scheduled follow-up phone calls to assess any difficulty and encourage them to keep the study procedures.
We expect these measures to promote retention and streamline individual participation to complete follow-up.
Data management
An ad hoc-created eCRF based on the Research Electronic Data Capture (REDCap) platform (REDCap Consortium) will be created in coordination with the Biostatistics Unit (UBiDi). Participants’ data will be anonymised.
We will comprehensively gather data regarding the inclusion date, sociodemographic data, medical history, relevant comorbidities, clinical data and information on any medication administered. Likewise, we will gather the relevant laboratory results when available.
Confidentiality
All trial-related documents will be treated under the European Regulation (EU) 2016/679 of the European Parliament and Council (27 April 2016) on Data Protection, as well as the Spanish Organic Law 3/2018 (5 December 2018) on the Protection of Personal Data and Guarantee of Digital Rights. Patient data will be pseudonymised.
Each study participant will be assigned a unique study number to ensure anonymity, which will be used in the eCRF. Regulatory authorities, trial monitors and auditors may have direct access to study data, if required, and will take all possible precautions to maintain confidentiality. The investigator shall ensure that the documents provided to the sponsor do not contain the patient’s name or any identifiable data.
Statistical methods
Primary and secondary outcomes
All collected variables will be summarised in tables using appropriate descriptive statistical methods (central tendency and dispersion measures, and absolute and relative frequencies, whenever applicable).
The main analysis (differences between baseline and EoT visits) will be conducted primarily in the intention-to-treat population; however, we will also analyse the per-protocol population. Pain intensity evolution will be assessed by determining the pain intensity, the pain intensity difference (PID), and the sum of the PIDs at each study visit. We will calculate the percentage of responders according to the definitions provided. We will perform bivariable contrasts between study groups of these endpoints by means of t-tests or Mann-Whitney U tests, and χ2 or Fisher’s exact test, as applicable.
Additionally, we will apply longitudinal data assessment methods based on mixed generalised linear models (Gaussian or Gamma, Poisson or negative binomial distributions for errors, as appropriate) taking the patient as a cluster. This will allow for assessing and comparing endpoints’ evolution over time, including the EoT and EoS follow-up visits. The independent variables will be the random intercept, the follow-up visit, the study group, the baseline value of the dependent variable, and the interaction between the visit and the study group. We will assess the interaction’s significance and plot each group’s marginal means at each visit (estimated by the models). These models will also be used for the advanced analyses to obtain estimates with causal interpretation (see the Additional analyses section). Improvement will be quantified by estimating the difference between the baseline and 28-day visits; the effect size will be estimated using the standardised mean difference (Cohen’s ‘d’).
The primary analysis will be replicated and adjusted to assess the role of sociodemographic factors, QoL, baseline social adaptation, clinical non-cancer disease variables and social support.
We will present tables with the model’s coefficients and their 95% CIs. Effect size measures will be provided with the marginal means per study group and their 95% CI.
We will replicate the raw and adjusted primary analysis for the EQ-5D-5L, SF-36, POMS, McGill and TMD questionnaires. The dependent variable of each model will be the respective response variables from this tool measured throughout the visits. Likewise, the estimated model will be replicated, adjusting for sociodemographic factors, baseline QoL, clinical variables of the non-cancer disease and psychosocial support.
The safety analysis will be performed in the safety population (ie, all included subjects who have taken at least one dose of opioids or have had at least one psychotherapy session). We expect the safety population to coincide with the total number of patients included in the study. Safety analyses will include a descriptive analysis of the AEs recorded throughout the trial for the whole population and stratified per study group.
Primary statistical analyses will be performed with R Statistical Software V.4.2 or higher (R Foundation for Statistical Computing, Vienna, Austria).
Additional analyses
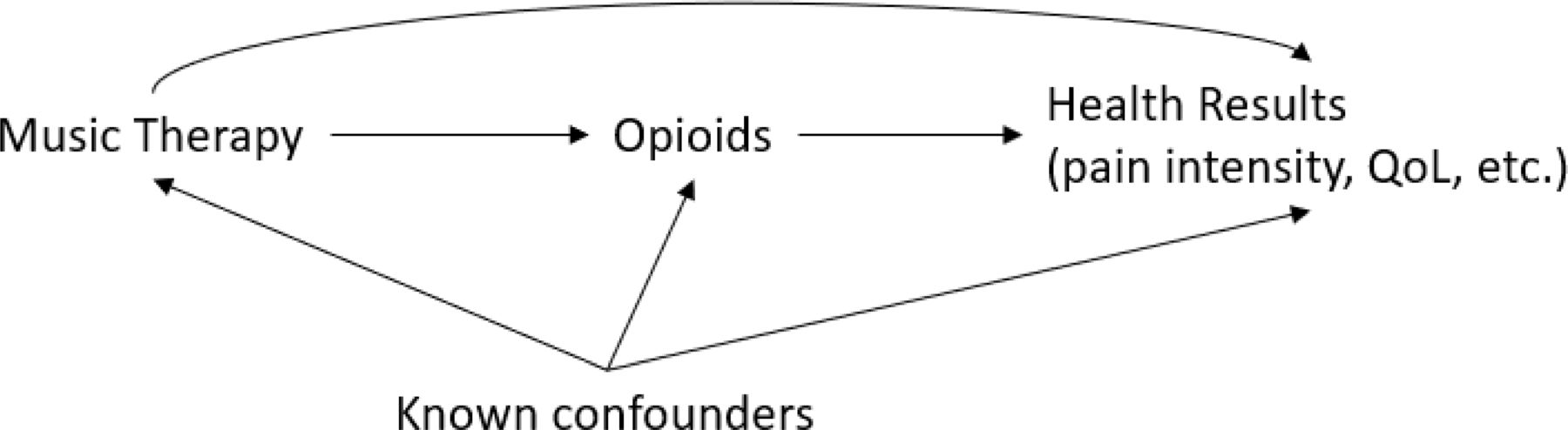
Although the study is randomised, we will apply statistical methods to obtain causal estimates to isolate the effect of music-listening within the context of other therapeutic measures that the participants will take simultaneously. For this purpose, we will perform mediation analyses based on the counterfactual outcomes framework to adjust for the effects of these additional therapeutic measures—whose interchangeability is not guaranteed by design since they are not randomised. Identification of causal estimates will be achieved by standardising the mean outcome to the confounder distribution by averaging the output after two rounds of the recursive g formula. The basic causal structure will be built around the therapeutic measure with the greatest expected effect (opioids) to structure music-listening’s direct and indirect effects. The basic causal structure is depicted in the directed acyclic graph provided in figure 2 and will use a four-way decomposition to assess the effects in the presence of interactions.54

{kind=link}
{kind=link}
Directed acyclic graph. QoL, quality of life.
Further details about this decomposition will be provided in a statistical analysis plan, including algebraic expressions for each expected effect. These analyses may be also extended by including additional paths to accommodate simultaneous mediator (opioid) intensities or the evaluation of other therapeutic interventions, such as rehabilitation or physiotherapy (if any).
Interim analyses are not planned for this study.
Methods in analysis to handle protocol non-adherence and missing data
We will apply two principles supported by the European Medicines Agency (EMA) for missing data imputation: (1) we will assume that the treatment effects’ estimates are unbiased and (2) that the overall probability of type I error is controlled.55 The mixed models planned for the analyses can accommodate random data missing mechanisms—that is, not specifically related to the interventions, which constitute a reasonable assumption in this study.
Composition of the coordinating centre and trial steering committee
This will be a single-centre study. The steering committee will be composed of the Head of the Chronic Pain Unit (AS), the Head of the therapists’ team (JG-S) and the Head of the Clinical Research Support Unit (SV).
While blinded, the trial steering committee will ensure the scientific integrity of the trial, the scientific validity of the study protocol, the assessment of study quality and conduct, and the scientific quality of the final study report.
Composition of the data monitoring committee, its role and reporting structure
The data monitoring committee will be composed of the person in charge of pharmacovigilance at our medical centre (Dr. Dolores Rodriguez-Cumplido), the person in charge of statistical analysis (Dr. Jesús Villoria) and a senior pain doctor (Dr. Maria-Victoria Ribera).
This committee shall assess the progress, safety data and, if needed, critical efficacy endpoints. The data monitoring committee may review unblinded study information (on a patient level or treatment group level) during the conduct of the study. It will provide the sponsor with recommendations regarding study modification, continuation or termination.
AE reporting and harms
The investigators will systematically follow-up and collect AEs from the moment participants sign the informed consent until the last follow-up visit. AEs will be registered in the participant’s medical record, as well as the causality assessment with the therapies under investigation. AEs and their causality assessment will also be registered in a specific eCRF section. They will be coded according to the latest available version of the MedDRA dictionary and will be described using absolute and relative frequencies by study group, according to severity and its causal relation with treatment.
All SAEs will be reported by the investigator with an ad hoc SAE Notification Form and emailed to the Sponsor within 24 hours of its fulfilment. The sponsor or its designee will evaluate the notification and may ask for additional information, if needed.
The sponsor will notify the Spanish Medicines and Health Products Agency (AEMPS) and the responsible health authorities of any suspected unexpected serious adverse reaction (SUSAR) associated with the therapies through the EMA’s EudraVigilance_CTM database; relevant Spanish Autonomous Communities should also be notified. The deadline for SUSAR notification to the AEMPS will depend on the reaction severity.
The sponsor may make an initial incomplete SUSAR notification to ensure celerity; however, a complete report shall be made no later than 8 days after the initial submission.
The sponsor will draft a regular annual safety update report according to the ICH-E2F guideline.56 These will be sent to the AEMPS, corresponding institutional review board (IRB), and responsible health authorities.
Ethics approval and consent to participate
The Bellvitge University Hospital IRB approved the study protocol, version 2.0 (Reference Number: PR026/23) on 30 March 2023. As per good clinical practice, we will inform the study participants of any significant changes during the clinical trial. Major protocol changes will undergo IRB approval; minor changes will be reported to the IRB.
The principal investigator or other study team investigator will explain the study to eligible patients and ask them to sign the informed consent form, if they wish to participate. All participants must sign the written informed consent prior to enrolment.
We do not plan to collect, use or store additional biological specimens. Therefore, no additional consents are planned.
Trial status
This trial is currently on the recruitment phase (May 2023).
Provisions for post-trial care
Study participants will continue their follow-up at the Bellvitge University Hospital Pain Clinic and will undergo medical tests and treatments prescribed according to standard clinical practice procedures.
Dissemination plans
This clinical trial is registered in the ClinicalTrials.gov database (NCT05726266), where the results will be published after the end of the trial, regardless of being positive or negative. Moreover, the results will be sent for publication on (preferably) English-language peer-reviewed medical journals and medical congresses. Publishing decisions will be taken jointly between the sponsor and the investigators.
The sponsor reserves the right to review any manuscript related to this study before its submission for publication. Neither party has the right to prohibit the publication unless proven that this publication affects possible patent rights. The sponsor reserves the right to postpone any scheduled publication until the approval of any patent application.
Plans to give access to the full protocol, participant level-data and statistical code
The protocol is available on ClinicalTrials.gov (NCT05726266). No public access to the patient dataset is planned at this moment. The corresponding author will oversee the dataset, and access to this information will be granted on a case-by-case basis and at the interested party’s request.
Plans for collection, laboratory evaluation and storage of biological specimens for genetic or molecular analysis in this trial/future use
We do not plan to collect or store biological samples during this trial.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the Bellvitge University Hospital, IDIBELL, and CERCA Program/Generalitat de Catalunya for institutional support. We also would like to thank Basetis S.A. for the pro-bono agreement for some of the work in the creation of the app used in this study.
References
Footnotes
JG-S, AS and JV are joint first authors.
AR-F, VF-D and SV are joint senior authors.
Twitter @grausanchezj, @AncorSerrano
Contributors JG-S, VF-D, SV and AR-F conceived the study design. AS, JV, TC and SV wrote the study protocol and the original draft. MFP, LZ, MF-G, AR-F, ES, JG-P, JG-S and VF-D provided clinical input and perspectives regarding the qualitative aspects of the study. AS, SV and VF-D coordinated ethics approval. All authors have read and approved the final manuscript version.
Funding This work was supported by the Neuroscience Program, IDIBELL-Bellvitge Institute for Biomedical Research, grant number 21VAR007, and by the Plan Nacional sobre Drogas (National Drugs Plan), grant number 2021I068.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.