Article Text

Abstract
Introduction Research suggests that current care for shoulder pain is not in line with the best available evidence. This project aims to assess the effectiveness, cost-effectiveness and the implementation of an evidence-based guideline for shoulder pain in general practice in Norway.
Methods and analysis A stepped-wedge, cluster-randomised trial with a hybrid design assessing clinical effectiveness, cost-effectiveness and the effect of the implementation strategy of a guideline-based intervention in general practice. We will recruit at least 36 general practitioners (GPs) and randomise the time of cross-over from treatment as usual to the implemented intervention. The intervention includes an educational outreach visit to the GPs, a computerised decision tool for GPs and a self-management application for patients. We will measure outcomes at patient and GP levels using self-report questionnaires, focus group interviews and register based data. The primary outcome measure is the patient-reported Shoulder Pain and Disability Index measured at 12 weeks. Secondary outcomes include the EuroQol Quality of Life Measure (EQ5D-5L), direct and indirect costs, patient’s global perceived effect of treatment outcome, Pain Self-Efficacy and Brief Illness Perception Questionnaire. We will evaluate the implementation process with focus on adherence to guideline treatment. We will do a cost–minimisation analysis based on direct and selected indirect costs and a cost–utility analysis based on EQ5D-5L. We will use mixed effect models to analyse primary and secondary outcomes.
Ethics and dissemination Ethics approval was granted by the Regional Committee for Medical and Health Research Ethics-South East Norway (ref. no: 2019/104). Trial results will be submitted for publication in a peer-reviewed medical journal in accordance with Consolidated Standards of Reporting Trials.
Trial registration number NCT04806191.
- shoulder
- musculoskeletal disorders
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Implementation of an evidence-based guideline for shoulder pain in general practice by using a tailored approach including educational outreach visits and a computerised decision tool for general practitioners (GPs) and a self-management application for patients.
The implementation will be supported according to the individual GPs needs based on systematic evaluation.
We will evaluate patient reported outcomes, cost-effectiveness and the implementation process.
Outcome measures and treatment content given by the individual GPs are mainly patient reported and is a potential limitation in the reporting of guideline adherence by GPs.
Introduction
Shoulder pain is a common reason for seeking the general practitioner (GP).1–3 Shoulder pain often results in sick leave and disability4 and complaints are often prolonged.5 6 To diagnose shoulder disorders is considered difficult and may be one of the reasons why GPs rely on radiographic examination in their assessment.7 8 It is recommended that the diagnosis is based on clinical examination.9 10 We define shoulder conditions through a set of criteria based on typical symptoms and findings.11 Traditionally, we have used biomedical and biomechanical explanations for causes of shoulder pain, which has formed the basis for our choice of treatment. However, research suggests a weak relationship between structural damage identified through radiological examinations and symptoms and prognosis.12 13 High-quality trials have documented that supervised exercises provide equally good results as surgical treatment for rotator cuff-related pain both in the short and long term and at a lower cost.14–16 Sham controlled trials question the efficacy of both surgery and exercises and a recent guideline emphasise proper information and shared decision making as base for treatment.16 Psychosocial factors, pain intensity and work-related factors are found to be the most important prognostic factors for improvement.17 18
The biopsychosocial model reflects the development of illness through the complex interaction of biological, psychological and social factors. Although the biopsychosocial approach is recognised, it is largely not adhered to in primary care according to a Canadian study.19 Changing clinical practice with the implementation of existing knowledge through clinical guidelines could provide a clinical and socioeconomic benefit through faster clarification, effective treatment at the right level in the health service and shorter sick leave for patients with shoulder complaints. Bridging the gap between evidence and patient care is challenging, and an in-depth understanding of barriers of implementation at different levels of healthcare is advocated.20 We consider it important that the GPs are strengthened in their ability to use simple and evidence based routines to distinguish the few who need specialist examination and at the same time confidently manage the many who benefit from simple measures implemented locally and immediately. Based on an evidence-based guideline for examination and treatment of shoulder pain in primary care,21 we have developed an electronic support tool for the GP with an information module for patients. To achieve an intervention that builds on up-to-date knowledge and is compatible with and useful in everyday life in general practice, the electronic decision tool was developed by GPs in close cooperation with patients and specialists. The intervention has been pilot tested in general practice and adapted before implementation and we present the protocol of a stepped-wedge cluster randomised study to test its effectiveness compared with treatment as usual (TAU).
Objectives
The primary objective of this study is to test the effectiveness of the implementation of a guideline-based complex intervention for the management of shoulder pain in general practice. We will examine clinical effectiveness at patient level by patient reported questionnaires concerning pain, disability, quality of life, self-efficacy and illness perception. Secondary objectives are to assess the cost effectiveness of the intervention and evaluate the implementation process with a focus on GPs and patient’s adherence to the evidence-based guideline. The implementation strategy will be examined at patient and GP level with a focus on adhering to the clinical guideline recommendations reported by questionnaires, logs of use of the computer software and qualitative interviews.
Hypotheses
We hypothesise that implementing the evidence-based guideline will, compared with TAU:
Reduce patients shoulder pain and disability measured by Shoulder Pain and Disability Index (SPADI).
Will be cost-effective measured by a cost–minimisation analysis (CMA) based on direct and selected indirect costs and a cost–utility analysis (CUA) based on the EuroQol quality of life measure (EQ5D-5L).
Improve quality of care defined as GPs adherence to the evidence-based guideline measured by reported treatment.
Methods and analyses
Study design
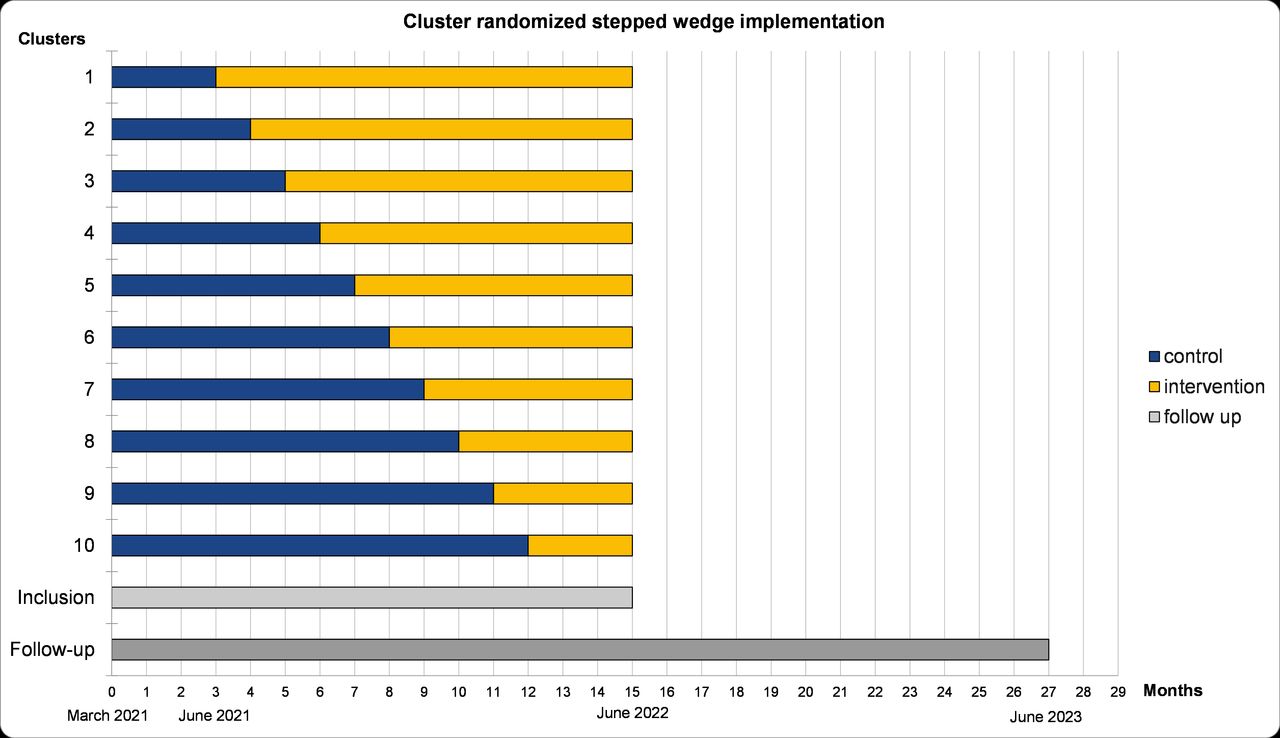
We will conduct a stepped-wedge, cluster randomised trial with a hybrid design assessing both clinical effectiveness and implementation of the intervention in clinical practice.22 Each GP surgery will be considered a cluster. The GP surgeries will switch from control (TAU) to intervention in a randomised order (figure 1). All clusters will be considered as controls (TAU) initially until the point of time when they cross over from TAU to the intervention. At the end of the inclusion period, all clusters will be using the intervention. Eligible patients will be recruited from the clusters without matching or stratification. Measurements at the patient and GP level will be undertaken simultaneously. GPs and patients will be invited to a qualitative interview to explore participants’ experiences regarding the implementation of the intervention.

{kind=link}
Timeline. Ten clusters representing each GP surgery. Recruitment of GPs ended in January 2021 and patient inclusion will start during March 2021. All clusters start as a control (blue) and will randomly be allocated to the intervention group (yellow). Implementation will start in June 2021 and will end in June 2022. Each patient is followed for 1 year. GP, general practitioner.
Setting
The study will be conducted in GPs surgeries in Norway. We will invite available GPs to participate in the study using the existing Norwegian Primary Care Research Network.23 We aim to include at least 36 GPs in both urban and rural settings. The study is a collaboration between the Department of General Practice at the University of Oslo (UiO), Norway, and the Department of Research and Innovation in Helse Fonna Health Trust in the Western Norway Regional Health Authority.
Recruitment of eligible patients with shoulder pain
The GPs and health secretaries in participating surgeries will ask patients presenting with shoulder pain for participation in the study. Posters with study information will be available in the GP surgeries. GPs are informed of inclusion and exclusion criteria and will register eligible patients name and phone number. GPs will start treatment the day the patient attend the surgery. The project coordinators will contact the surgeries twice weekly for patients’ names and phone number. The study coordinators will then contact the patients to provide study information and perform a supplemental screening in relation to the inclusion and exclusion criteria and comorbidity by telephone (table 1). Patients that comply with the criteria will then receive the written information material and consent form electronically by logging in to an electronic platform. Patients who do not meet eligibility criteria or decline participation will receive TAU by their GP. If the study coordinator is in doubt whether the patient is eligible according to the criteria, the coordinator will contact the GP and discuss the matter. We will gather information about gender, age and if possible, the reason for declining participation for patients not entering the study to assess the generalisability of the trial.
Inclusion and exclusion criteria
Intervention
The intervention is based on a Norwegian guideline for treatment of non-traumatic shoulder pain in general practice.21 The guideline is grounded in a biopsychosocial model of medicine with a goal of reaching cognitive reassurance through adequate clinical examination, information and intervention on key prognostic factors. We have had an overarching goal to simplify the guideline to an easy intervention suiting the clinical everyday life of the GP. We will introduce the intervention to the GPs in outreach workshops. The content of the intervention is available to the GPs as an electronic decision support tool (EDT). The EDT is a downloadable computer software for the GPs which can interact with a patient information application (PIA) for smartphones.
We used the Website Development Model for the Healthcare Consumers (WDMHC) for development of the EDT and the PIA.24 The WDMHC ensures user participation and a usability evaluation. In 2019/2020, we have conducted a pilot study to assess the feasibility of the procedures in order to improve the planned study. In an iterative process with 10 patient interviews and 5 focus group interviews with 21 GPs, the information material and electronic applications were further developed and refined. We will conduct a user evaluation to further improve the tool.
The GP workshops and the EDT
A 3-hour workshop will be arranged at the GPs offices with a goal of teaching participating GPs to examine and treat patients with shoulder pain according to the Norwegian guideline for treatment of non-traumatic shoulder pain in general practice. Main content of the workshops is listed in table 2. The workshops will introduce the EDT and its use in clinical practice. The EDT will be an accessible information base for GPs with recommendations on how to examine, treat and follow-up patients with shoulder pain at different stages (table 2). Recommendations are presented in text, illustrations and videos. Advocating a shared decision-making process with patients, GPs will be able to find important information topics for the patients and make a targeted electronic information package to the patient.
Content of the intervention
The patient information application
Patients recruited in the intervention phase of the study will get access to the PIA for use on their smartphone. The GPs will be able to tailor information to the individual patients based on the patients information needs revealed under the consultation. Available content is shown in table 2. The patient information is in text, illustrations and videos. For patients not using a smartphone, a written leaflet can be printed out and handed to the patients. The leaflet also contains a link to the patients’ internet site accessible from a home computer.
Randomisation and blinding
We will randomly allocate the GPs surgeries to one of the 10 time points for crossing over from control group to the intervention group using a computer-generated list of random numbers. Randomisation will be performed after the recruitment of the GP surgeries. GPs, workshop and study coordinators and outcome evaluators will be blinded to the allocation sequence with only the next GP surgery being revealed by randomisation list holder approximately 6 weeks before each intervention implementation point. GPs and patients will not be blinded for group allocation. The project coordinators and the personnel responsible for the workshops will not be blinded, but the primary study statistician and health economist will be blinded for group allocation.
The control phase
In the control phase, participating GPs are informed of the study, but the GPs have not yet attended the workshop and do not have access to the EDT or the PIA developed for this study. Patients will be treated as usual by their GPs.
The intervention phase
Workshops for GPs will be arranged at the GP surgeries at the time point for switching from control to intervention group for each participating GP surgery (table 2). After the workshop, the GPs will be asked to implement the intervention as taught at the workshops. We will do implementation supportive interventions tailored to GPs needs based on their score using a validated questionnaire 2 weeks after the workshop (implementation process assessment tool (IPAT)).25 As an example, clinicians giving a low score on being confident in the new method or had doubts about the gains for patients will be contacted by a peer project coordinator to discuss the matter. Each intervention is tailored to the GP’s needs and based on theoretical concepts such as readiness for change and stages of change. The project coordinators will also ensure that electronic decision tools and patient material works as planned.
Data collection
We will collect demographic data and prognostic factors at baseline. Primary and secondary outcome measures, costs and healthcare consummation will be gathered additionally at 6, 12 and 52 weeks. Implementation outcomes will be registered at all-time points. A detailed description of the different variables are given in table 3.
Data collection
We will ask the patients to complete electronic questionnaires via a link sent by email using an electronic automated questionnaire with a reminder function developed and operated by the University Information Technology Centre at UiO specifically designed to meet Norwegian privacy requirements. All data will be set up for direct encrypted delivery to secure storage in the UiO Services for Sensitive Data. If a patient has no email address or internet access or is reluctant to reply electronically, the questionnaire and a prepaid envelope will be mailed to the patient. Project coordinators will collect information on patient age, gender and comorbidity during the telephone screening. Other patient characteristics and shoulder related information will be self-reported at baseline (table 3). Demographic data on the GPs will be collected after recruitment (table 3). If patients or GPs do not respond to follow-ups, a reminder email will be automatically sent by the electronic automated system. Telephone follow-up will be used to patients not responding to multiple email reminders. One project coordinator will have full access to research data and routinely check the data quality.
Primary outcome measure
Primary outcome measure is the SPADI measured at baseline, 6 weeks, 12 weeks and 52 weeks (table 3). The primary time point of interest for the SPADI score is at 12 weeks. SPADI is a self-reported questionnaire with 13 items regarding shoulder pain and disability. SPADI has been used and validated in primary healthcare,26 is cross-cultural translated to Norwegian27 and is regarded as easy to understand and report by patients.
Secondary outcome measures
Secondary outcomes (table 3) will include: The patient reported EQ-5D-5L score measuring health related quality of life on the five domains mobility, self-care, usual activities, pain and discomfort, and anxiety and depression as well as the general health condition using the EuroQol Visual Analogue Scale (0–100). We will use a single seven-point scale to measure global perceived effect of treatment outcome. Psychological factors will be measured using the Pain Self-Efficacy Questionnaire (PSEQ) and the Brief Illness Perception Questionnaire (BIPQ). The PSEQ is a 10-item questionnaire assessing the confidence people with ongoing pain have in performing a range of functions, including household chores, socialising, work, as well as coping with pain without medication. The BIPQ is a nine-item patient reported questionnaire designed to rapidly assess the cognitive and emotional representations of illness. We will measure health resource use (consultation with primary and secondary care, prescribed and over-the-counter medication use, physiotherapy or other therapies, alternative therapy, radiology, hospital admission and treatment in secondary healthcare; travel expenses, production loss and work absence (number of whole sickness days). All costs will be patient reported by questionnaire. Additionally, sick leave data will be obtained from the Norwegian Labour and Welfare Administration registry.
Implementation of the intervention
Based on elements of the conceptual framework for implementation fidelity28 and the Medical Research Council guidance on process evaluation on complex interventions,29 we will do a process evaluation with focus on GPs and patients adherence to the intervention. We will evaluate GPs adherence to guideline directly by analysing treatment content reviewing patient’s medical records and indirectly by analysing patient’s reports on six items regarding key elements of the guideline measured on five point Likert scales. The six items are: received information about your shoulder pain; being examined by your doctor; received an explanation of your shoulder pain; received written information about shoulder pain and treatment; elaborated a plan for self-management of shoulder pain and discussed different treatment options with your GP (pain medication, cortisone injection, shoulder exercises and referral to physiotherapist). We will evaluate patient’s adherence by reviewing logs of use of the PIA-software and reported treatment (information, medication and frequency of exercises). We will assess GPs readiness for change and stages of change by using the IPAT25 at 2 and 12 weeks after the workshop. We will assess GPs confidence in handling patients with shoulder pain using a nine-item questionnaire measured on six-point Likert scales based on important elements of the guideline (information, clinical examination, clinical diagnosis, referral to radiology, pain medication, cortisone injection, shoulder exercise, prognostic factors, referral to secondary care). GPs and patients judgement of benefit, satisfaction and usability of the different components of the intervention (workshop, the EDT software, PIA software) will be assessed (table 3). We will ask included GPs and patients to participate in individual or group focus interviews to explore participants’ experiences during the trial with attention to barriers and facilitators of using the intervention.
Sample size
The target sample size is 250 patients. The incidence of shoulder pain in general practice has been reported to be 2%–4%.1 2 Based on the ICPC-2 codes for shoulder pain, we found that 67 patients were given a primary shoulder diagnosis in a GP surgery with three GPs in Østfold County in Norway in 2017. Most GP surgeries have three to four GPs in Norway. Therefore, in estimating the sample size for this study, we used a conservative assumption of 3% as the incidence of shoulder pain. Previous studies guided our choice of estimates for the sample size calculation. We used the computer programme IBM SPSS Sample Power V.3.01 and inflated by the design effect using the formula  where n is the number of individuals per clusters and ρ the intracluster correlation coefficient (ICC).30–33 Setting the desired statistical power of the study at 80%, alpha at 0.05 for a two sided test and an ICC of 0.02, we estimated that we needed to recruit 250 patients to detect a clinically important difference of 8 points between the groups in the SPADI score and an SD of 22 points in both groups, taking into account a possible drop-out rate of 10%. Thus, assuming that only one-third of the patients contacting their GP will participate in the study, we will recruit at least 36 GPs in 10 GP-clusters to recruit an adequate sample size in 1 year. We will if necessary, increase the recruitment period to reach an adequate targeted sample size.
where n is the number of individuals per clusters and ρ the intracluster correlation coefficient (ICC).30–33 Setting the desired statistical power of the study at 80%, alpha at 0.05 for a two sided test and an ICC of 0.02, we estimated that we needed to recruit 250 patients to detect a clinically important difference of 8 points between the groups in the SPADI score and an SD of 22 points in both groups, taking into account a possible drop-out rate of 10%. Thus, assuming that only one-third of the patients contacting their GP will participate in the study, we will recruit at least 36 GPs in 10 GP-clusters to recruit an adequate sample size in 1 year. We will if necessary, increase the recruitment period to reach an adequate targeted sample size.
Data management
All electronic data will be automatically and safely stored on research servers in accordance with the regulations of the Norwegian Center for Research Data and the UiO. Any written data will be stored securely and locked in the trial coordinator office at the UiO until transferred to an electronic format on the research servers. All documents, except written consent and patient contact details, will refer to the patients with a unique study participant number and not by name. Data will be retained de-identified for 5 years as demanded by EC/REK southeast. Data will then be anonymised.
Statistical analysis
We will analyse the difference between the TAU and intervention groups in the mean SPADI score to the principle of intention to treat. We will use mixed effects regression models with random effects at GP and patient levels to analyse repeated measurements of both the primary and secondary outcomes. Estimates of ICC, which measures the amount of variability in SPADI due to differences between GP surgeries and between patients, will be obtained from the mixed effects regression models. Statistical significance will be set at the 5% level and we will report 95% CIs of effect sizes. We will summarise and report the patterns and types of missing data and explore the possibilities of multilevel multiple imputation if missing data exceed 10%.
Cost-effectiveness
We will use two methods to assess the cost-effectiveness of the intervention, that is, CMA and CUA. For the CMA, we estimate the direct costs in the health service (consultations, treatments, assessments, medication, surgery) and selected indirect costs (travel costs and productivity).34 Sick leave will be analysed as days away from work, that is, part time sick leave will be summed up whole days away from work. Both total and shoulder specific work absence will be analysed using patient reported and registry data.35 Direct and indirect costs are compared for intervention and TAU groups, respectively. In addition, based on the same costs, a CUA will be performed where the costs per quality-adjusted life-years are compared for the two options. The health-related quality of life scores for the alternatives are calculated using EQ5D-5L at baseline, 6 weeks, 26 months and 52 weeks. The economic evaluations will be based on decision-analytic modelling and we plan to do deterministic and probabilistic sensitivity analysis for both analyses.
Implementation
We will treat the patient’s reports on the six items on key elements of the guideline as individual items and we will compare the scores between the groups. We will dichotomise the sum score of the six items (0–24) and scores at or above 18 points (3 or more on each item) will be considered consultations of high adherence related to content according to the treatment guideline. The difference in proportions of high adherence to guideline treatment will be compared between groups under the null hypothesis that there is no difference between groups. We will report logs from use per patient of the EDT software and analyse the patients’ medical journal as supplementary information on the same key elements. Patients’ adherence to the treatment plan will be analysed by evaluating patient reported items on use of PIA, use of medication and exercises. We will also report logs of use of the PIA. We plan to do focus group interviews of selected GPs and individual patients in the intervention group for a thorough evaluation of barriers and facilitators of using the EDT and PIA. We will analyse the implementation process of the intervention from the GPs perspective using the IPAT-questionnaire at 2 and 12 weeks. An exploratory analysis of individual IPAT items will be presented as descriptive data and used to facilitate the implementation process tailored to the GPs needs. An exploratory analysis of relationships between IPAT scores, use of the EDT-software, the GPs satisfaction, and perceived benefit with use of the intervention and patient reported clinical results will be investigated. We will measure patients’ PSEQ, illness perception and outcome expectations. Exploratory analyses of relationships between these factors and use of the PIA, satisfaction with treatment, perceived benefit of treatment and patient reported clinical results will be investigated.
Discussion
With the EASIER study, we aim to investigate the effectiveness of a new evidence-based guideline of handling shoulder pain in general practice compared with TAU. Secondary aims include evaluating cost-effectiveness and the implementation process of using educational outreach workshops and an EDT and PIA-tool to implement the guideline in clinical care. This large cluster stepped wedge randomised trial will add to the current knowledge on structured approaches aiming to improve the uptake of evidence-based care for shoulder pain in primary healthcare and these results may be transferable to other musculoskeletal disorders.
We are aware of some limitations in this study. The cluster randomised design is susceptible to selection bias because of the difficulty in blinding study recruiters or potential subjects to the allocation of their cluster prior to consent. However, we will be able to identify differences in important baseline characteristics and prognostic factors at baseline. Most outcome measures and type of treatment content given by the individual GPs are patient reported and this is a potential limitation in the reporting of guideline adherence by GPs. Also, the retrospective reporting of healthcare use will be exposed to recall bias.
We believe this targeted implementation model may increase use of evidence-based methods for treating shoulder pain, improve the quality of care and hopefully the clinical results for patients.
Patient and public involvement statement
Patients and GPs have taken part in the development of the intervention and will contribute with their experiences of using the intervention. Patients and GPs has not been involved in design, choice of outcome measures or conduct of the study.
Ethics and dissemination
Ethics approval was obtained from the Regional Committee for Medical and Health Research Ethics (ref. no: 2019/104 REK Southeast C). Any modifications to the protocol which may impact on the conduct of the study will require a formal amendment to the protocol. Such amendment will be agreed on by the research group and approved by the Ethics Committee/REK southeast prior to implementation and communicated to relevant parties. We will collect the data in compliance with the Good Clinical Practices protocol and the Declaration of Helsinki principles. Patients and GPs will receive written and oral information about the study. Written informed consent will be obtained prior to baseline data collection with emphasis on the right to withdraw from the study at any time without any explanation. Public access to the full protocol, dataset and statistical code can be made available on request. Trial results will be submitted for publication in a peer-reviewed medical journal in accordance with Consolidated Standards of Reporting Trials.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors OME, SJP, BN, JIB, EKB, SER, KBE, PJ, IM and NGJ contributed to the development and design of the study. SJP, OME, NGJ and BN will carry out the study. NGJ, SJP and OME will coordinate the study. OME drafted this manuscript. All authors critically read and modified the study protocol and previous drafts of the manuscript and approved the final version.
Funding This work was supported by the Western Norway Regional Health Authority grant number F-11517 and the Norwegian Research Fund for General Practice.
Disclaimer This funding source had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.