Article Text

Abstract
Objective Even though 32%–83% for fear of falling (FoF) in patients with stroke, very little is known about the predictors of the problems. Therefore, we systematically reviewed the literature on risk factors for FoF in patients with stroke.
Design A systematic review and meta-analysis
Data sources PubMed, Embase, Cochrane Library database, Web of Science, CINAHL, PsycINFO, Grey literature and other relevant databases for related publications were searched (from inception to 17 July 2021).
Results Eight studies involving 1597 participants were selected to analyse risk factors for patients with stroke with FoF. The quality of all included studies was assessed and categorised as medium or high quality. Review Manager V.5.3 merged the OR value and 95% CI of the potential risk factors. Meta-regression and Egger’s test were performed by Stata V.15.1. The risk factors for FoF in patients with stroke were women (OR=2.13, 95% CI 1.47 to 3.09), impaired balance ability (OR=5.54; 95% CI 3.48 to 8.81), lower mobility (OR=1.12; 95% CI 1.05 to 1.19), history of falls (OR=2.33; 95% CI 1.54 to 3.53) and walking aid (OR=1.98; 95% CI 1.37 to 2.88), anxiety (OR=2.29; 95% CI 1.43 to 3.67), depression (OR=1.80; 95% CI 1.22 to 2.67), poor lower limb motor function (OR=1.14; 95% CI 1.00 to 1.29) and physically inactiveness (OR=2.04; 95% CI 1.01 to 4.12). Measurement of heterogeneity between studies was high for all outcomes (I2=0%–93%), indicating that the substantial interstudy heterogeneity in estimated proportions was not attributed to the sampling error. Sensitivity analysis (leave-one-out method) showed that the pooled estimate was stable.
Conclusion This meta-analysis indicated that female population, impaired balance ability, lower mobility, history of falls and walking aid in patients with stroke might be at greater risk for FoF. Future studies are recommended to determine other risk factors specific to patients with stroke.
- Stroke
- GERIATRIC MEDICINE
- Neurology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study has been reported per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting checklist.
Reported risk factors of fear of falling in patients with stroke using validated screening tools.
Searches included published and unpublished sources of literature to reduce the risk of omitting potentially eligible data.
Many risk factors were examined by a single study, thereby limiting our ability to meta-analyse these potential risk factors.
The variability in methods of assessing risk and reporting the frequency of risk characteristics limited analyses.
Introduction
Stroke is the second leading cause of death worldwide,1 creating a serious burden on caregivers.2 3 In 2010, an estimated 16.9 million stroke incidents occurred, increasing the number of 33 million stroke survivors all over the world.4 As a result, there were 5.9 million people who died, whereas 102 million people with disability-adjusted life years were lost because of the stroke.
On the other hand, it is well known that stroke can cause physical damage, such as weakness, paralysis, sensory disturbances, impaired postural control,5 mental fatigue, depression and impaired cognitive function.2 6 According to the WHO,7 a fall is defined as ‘an event which results in a person coming to rest inadvertently on the ground or floor or other lower level, with or without injury’. Both physical and mental impairments can contribute to a fall, a common complication after a stroke.8 Among those who survived a stroke, 22%–48% have experienced at least one fall in the hospital8–10 or the rehabilitation facility.11–13 There is a reported prevalence of 32%–83% for fear of falling (FoF) between the first 6 months and just over 4 years after stroke onset.14
A high level of FoF psychology that limits the patient’s active rehabilitation exercise behaviour reduces their mobility, flexibility and independence and increases their anxiety and depression.15 The FoF psychology hinders the recovery of the adults’ physical and mental functions, thereby increasing the risk of falling and forming a vicious circle.16
In clinical practice, identifying FoF risk factors in patients with stroke is more helpful in guiding clinical practice. Many reports have mentioned that identifying the FoF status of patients with stroke and strengthening the comprehensive interventions in this field can plausibly help break the vicious circle, relieve anxiety,17 promote community reintegration18 and improve the quality of life.19 Some previous studies have proposed the correlation between many potential risk factors and FoF, intervention measures to reduce FoF incidence during stroke and risk factors for falls in patients with stroke.20 However, the risk factors identified for FoF in different studies are inconsistent. These reports have neither comprehensively explored sociodemographic, psychological and physical risk factors, nor included systematic reviews and meta-analyses of risk factors for FoF in patients with stroke.21–23 Therefore, we conducted this systematic review and meta-analysis to identify risk factors for FoF in patients with stroke.
Methods
Search strategy
We searched PubMed, Embase, Cochrane Library, Web of Science, CINAHL, PsycINFO, Grey literature and other databases (from inception to July 2021) for studies that identified risk factors for FoF in patients with stroke.
Our search strategy used medical subject heading and natural language text words. The first author designed specific search strategies and peer-reviewed electronic search strategies. The specific search strategy for each database is mentioned in online supplemental file 1. References from relevant papers or reviews were hand-searched for additional studies. For missing relevant data from studies, we contacted the study’s authors via email. All studies that were classified as FoF studies were then screened. On 20 July 2021, another search was performed on the previously mentioned database to search the articles published since the initial examination date.
Supplemental material
Inclusion and exclusion criteria
The inclusion criteria: (1) published case–control studies, cohort studies and cross-sectional studies; (2) all participants 18 years and above and clinically diagnosed with either first stroke or recurrent stroke; (3) studies published in the English or Chinese language; (4) reported risk factors of FoF in patients with stroke using validated screening tools, (5) the data can be extracted, including the spreadsheet of the pretest in the study.
The exclusion criteria: (1) review papers, case reports, meeting abstracts, qualitative studies; (2) duplicate literature or research with the same data; (3) research on quality evaluation results is low.
Endnote X V.9 software was used to remove duplicates and facilitate the screening process. All titles and abstracts were screened for inclusion/exclusion based on the eligibility criteria. The full texts were evaluated if the title and abstract could not accurately identify the possibly eligible studies (online supplemental file 2).
Supplemental material
Data extraction and quality assessment
The literature extraction was independently conducted based on the search, reviewed and selected according to predefined criteria. The data were collected from studies: first author, year of publication, geographical location, the measured/collected tools, study type, research period, total sample size, sociodemographic data and risk factors. The odds ratio (OR) or the risk ratio (RR) and its 95% CI was directly extracted from the included studies. All the information was recorded in especially standardised forms. For the missing relevant data of studies, we contacted the study’s authors via email; however, if the relevant data could not be obtained, the study was excluded (online supplemental file 3).
Supplemental material
The methodologic quality assessment of case–control studies and cohort studies was assessed by the Newcastle Ottawa Scale (NOS)24 for the study population (four items), comparability (one item) and outcome evaluation (three items). The scale’s total score was kept as 9 points, where 0 to 3 were divided into low-quality research, 4 to 6 were divided into medium-quality research and 7–9 were divided into high-quality research. In addition, the risk of bias in a cross-sectional study was assessed using the instrument Agency for Healthcare Research and Quality (AHRQ).25 The tool had a total of 11 items as follows: if the answer to an object was ‘no’ or ‘UNCLEAR’, the item’s score was ‘0’; if the answer was ‘yes’, the item score ‘1’, with a total score of 0–11 points, 0–3 points=low quality, 4–7 points=medium quality, 8–11 points=high quality.26 The process of study selection, data extraction and quality assessment were all conducted in duplicate (Q Xie and JH Pei) with third-party adjudication (XM Dou) for disagreements.
Statistical analysis
To assess the risk factors of FoF, we conducted a meta-analysis by the RevMan V.5.3 software to pool the OR/RR value with 95% CI. Meta-regression and Egger’s test were performed by the Stata V.15.1, whereas all other statistical analyses were conducted with the RevMan V.5.3 software. Statistical heterogeneity between studies was quantified by the I2 statistics and formally tested by Cochran’s Q statistic. A random-effects model for meta-analysis was an obvious conservative choice based on the heterogeneity of geographic settings and the variability of screening and diagnostic tools. However, when the number of studies was small (n<5), a fixed-effects model was used.27–29 The findings were illustrated in the form of forest plots. Publication bias was identified using a funnel plot and Egger’s test.30 We planned to conduct subgroup and meta-regression analyses based on sample size and proportion of women.31 As previous studies have shown that SwePASS scores and age were influencing factors, we performed the post hoc subgroup and meta-regression analyses on these two factors when the number of studies >2.31–33 Statistical significance was set at p value <0.05. Sensitivity analyses were performed using the leave-one-out method.
Patient and public involvement
No patient was involved in the study.
Results
Literature selection
Initially, 2731 records were searched from the six databases and other resources (figure 1). After the exclusion of duplicates, the remaining 1646 records were screened. After analysing the title and abstract, ultimately, 92 publications were selected for the full-text assessment. Finally, eight full-text studies with 1597 participants were found eligible and included in this meta-analysis.

Flow diagram of study selection in the meta-analysis.
Study characteristics and methodologic quality
The included eight studies were conducted in three regions, that is, Asia (n=4), North America (n=1) and Europe (n=3). Among these eight studies, two were cross-sectional, four were case–control and two were prospective cohort studies. A summary of literature characteristics used in the analysis is shown in table 1.
Characteristics of the included studies
The NOS assessed the quality of the case–control studies and prospective cohort studies. The NOS scores ranged from 7 to 9, indicating a high level of studies quality. In the two cross-sectional studies, the AHRQ scores ranged from 4 to 6, indicating a moderate level of quality. The overall score indicated the relatively high quality of the literature included in this study.
Results of the meta-analysis
Sociodemographic factors
Three of the eight studies reported the relationship between sociodemographic factors and FoF, whereas the two reported predictors were age and women. Due to the limited number of studies, the ability to assess the publication bias by the funnel plot and Egger’s test was unsuccessful.30
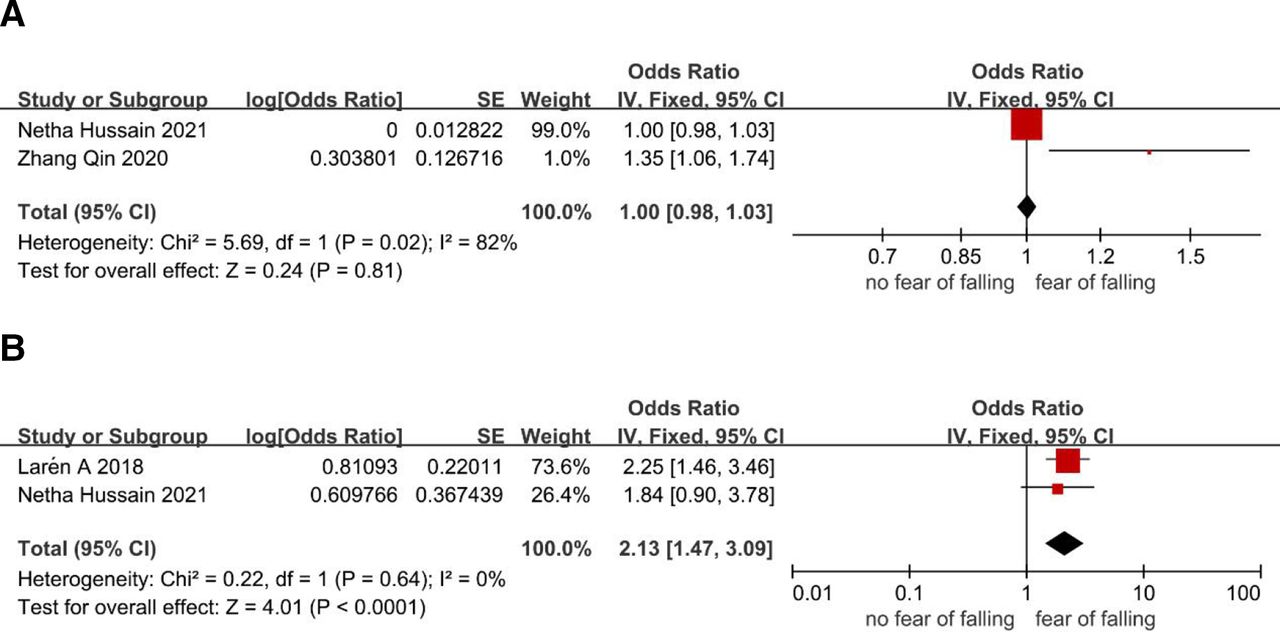
Age
Two studies with 500 participants reported the relationship between age and FoF in patients with stroke. Meta-analysis using a fixed-effects model showed that there was no statistically significant association (OR=1.00, 95% CI 0.98 to 1.03, p=0.81, I2=82%; figure 2A).

Meta-analyses for the association between sociodemographic factors and fear of falling: (A) age, (B) female gender. The solid vertical line indicates no effect. The solid squares indicate the mean difference and are proportional to the weights used in the meta-analysis. The diamond indicates the weighted mean difference, and the lateral tips of the diamond indicate the associated confidence intervals (CI). The horizontal lines represent the 95% CI.
Women
Two studies with 741 participants reported the correlation between women and FoF in patients with stroke. A pooled analysis using a fixed-effects model demonstrated that women experienced a significantly higher incidence of FoF than men (OR=2.13, 95% CI 1.47 to 3.09, p<0.0001, I2=0%; figure 2B).
Physical factors
Balance ability
Three studies reported the correlation between balance ability and FoF14 34 35 (911 participants). Based on the meta-analysis of the three studies on the risk factors of FoF, the results show large heterogeneity (p=0.003, I2=97%). The sensitivity analysis revealed clinical heterogeneity from different assessment tools. Ying et al34 measured balance ability with the Berg Balance Scale (BBS) score, whereas Larén et al14 and Hussain et al35 defined it by using the SwePASS score (postural control). Subgroup analysis of the SwePASS score showed that patients with stroke with lower balance levels were significantly more susceptible to FoF than higher balance levels (figure 3A). The results showed that the risk of FoF with a SwePASS score <24 (OR=5.54; 95% CI 3.48 to 8.81; I2=86%) was higher than a SwePASS score 25–30 (OR=2.30; 95% CI 1.47 to 3.58; I2=0%). This subgroup difference was statistically significant (p=0.007). There was no evidence of publication bias based on the Egger’s test (p=0.135).

Meta-analyses for the association between physical risk factors and fear of falling:(A) balance ability and (B) mobility.
Mobility
A meta-analysis using a fixed-effects model included three studies on the risk factors of FoF (377 participants) demonstrated a significantly higher incidence of FoF in lower mobility patients with stroke (OR=1.12; 95% CI 1.05 to 1.19; figure 3B) and revealed a considerable heterogeneity between the studies (p=0.0003, I2=84%). Meta-regression was performed to explore potential sources of heterogeneity based on an a priori list of factors related to clinical prognosis.33 Meta-regression analysis showed subgroup effects for age (p interaction =0.017), sample size (p interaction =0.019) and proportion of women (p interaction =0.019). Sensitivity analysis (leave-one-out method) showed that the pooled estimate was stable. In addition, there was no evidence of publication bias according to a funnel plot (online supplemental file 4) and the Egger’s test (p=0.619).
Supplemental material
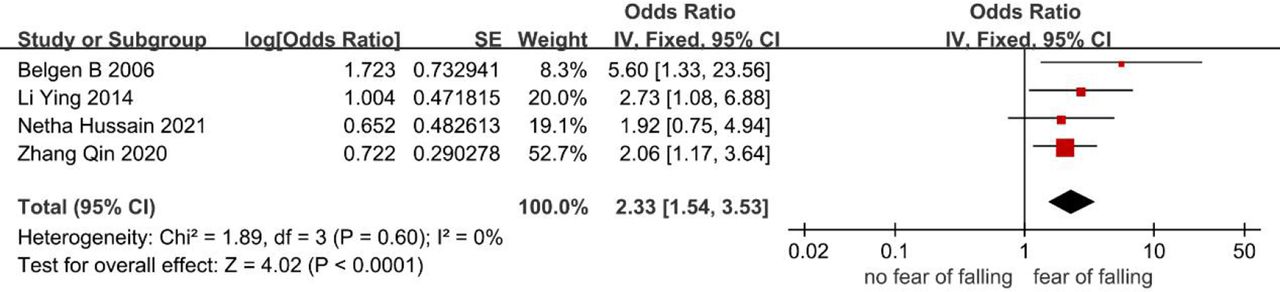
History of falls
Four studies reported the correlation between experience of falls and FoF34–37 (720 participants). Furthermore, Watanabe38reported that 87.9% of those who have experienced a fall would have a FoF for patients with stroke. Fixed-effects model analysis included four studies that revealed that the risk of FoF in patients with stroke with a history of falls was 2.33 times higher than no falls (OR=2.33; 95% CI 1.54 to 3.53; I2=0%; figure 4). There was no evidence of publication bias according to a funnel plot (online supplemental file 5) and the Egger’s test (p=0.205).
Supplemental material

Meta-analyses for the association between history of falls and fear of falling.
Use of walking aid
Two studies listed the relationship between the walking aid for patients with stroke and FoF14 35 (741 participants). Larén et al14 reported valuable insight into those involved in stroke rehabilitation during the acute phase after stroke. FoF was associated with the use of a walking aid, whereas Hussain et al,35 using the multivariable regression model, showed that the walking support for FoF was not statistically significant. A meta-analysis using a fixed-effects model that included two studies revealed that the risk of FoF in patients with stroke who used a walker is 1.98 times that of those who did not use a walker (OR=1.98; 95% CI 1.37 to 2.88, I2=93%; figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analyses for the association between using walking aid and fear of falling.
Other risk factors
Only six factors were assessed in more than one study and found eligible for meta-analysis. All other risk factors estimated are described narratively based on the findings of the associated individual study. Among them, anxiety (OR=2.29; 95% CI 1.43 to 3.67), depression (OR=1.80; 95% CI 1.22 to 2.67), poor lower limb motor function (OR=1.14; 95% CI 1.00 to 1.29) and physically inactiveness (OR=2.04; 95% CI 1.01 to 4.12) increased the risk of FoF in patients with stroke.
Qin et al36 and Schmid et al39 reported that anxiety, depression and marital status were some of the risk factors for FoF. Specifically, marital status with a spouse was protected against the development of FoF. Yadav et al40 identified that every 1 unit increase in lower extremity Fugl-Meyer score had a 1.36 times chance of a person belonging to no FoF group. Thus, improving the lower extremity motor function can reduce the chances of belonging to no FoF.
Furthermore, Schinkel-Ivy et al41 reported that FoF was positively correlated to the walking velocity in individuals with stroke. This research used a 4.6-meter-long pressure pad system (Gaitrite, CIR Systems, Clifton, New Jersey) to measure gait, where walking velocity and double support time were used as an outcome indicator.42 Data on other risk factors are found in table 2.
Detailed data on other risk factors for the patient of FoF after stroke
Discussion
This study included observational studies with 1597 stroke participants. Out of the eight studies, two were cross-sectional studies, four were case–control studies, and two were prospective cohort studies with a wide range of patient characteristics. Furthermore, the reliability of the results was confirmed by the sensitivity analysis. This meta-analysis revealed that the female population, impaired balance ability, lower mobility, the experience of falling and walking aid were strongly associated with FoF among stroke individuals. Pooled results of these eight studies and another meta-analysis on fall risk factors in community stroke survivors20 were consistent for reduced balance (OR 3.87),20 depression (OR 2.11)20 and history of falls associated with the falls and FoF. Furthermore, this study showed the history of fall lead to a higher risk of FoF in patients with stroke (OR 2.33) than in falls (OR 1.67).20 Similarly, the reduced balance was more likely to contribute to the FoF. The present study’s findings highlighted that having a history of falls, either in-home, in the community or hospital setting, have a higher risk of recurrent falling in the stroke group (OR 4.19) than in the older community. In addition, in concurrence with another systematic review study about the risk factors of FoF in the elderly,43 our analysis also revealed that the problems of fall history and gait were related to FoF. Furthermore, our study highlighted that having a history of falls indicates that the risk of falling fear in the stroke group (OR 2.33) was higher than that of the elderly (OR 0.21).
The relationship between balance ability and FoF was further analysed. For example, Oguz et al44 found a strong negative correlation between objective balance (measured by BBS scores) and Fall Efficacy Scale (FES) scores (r=−0.808); however, there was a strong positive correlation between perceived sense of balance and FES score (r=0.714). Furthermore, the present study’s balance ability and mobility analysis results were in-concurrence with the study of Cho et al,45 who showed that the FoF and they were positively correlated (respectively, r=0.669; r=0.545). Other studies, such as Akosile et al,46 showed a negative correlation between physical function and fall efficacy (r=−0.66). Kim et al19 revealed that the physical factors, including the functional ambulation category, hip abductor strength, knee extensor and ankle plantar flexor had a negative correlation with FoF (respectively, r=−0.673; r=−0.534; r=−0.478; r=−0.501). Of note, the above results are contrary, which can result from different statistical analyses and research focuses used in these studies. Further, gait speed was related to the ability to maintain balance, where gait disorders limited the independent life of patients with stroke.47 Due to reduced weight transfer capacity and stability, many stroke survivors might find it challenging to maintain their balance.47 A previous study showed that the stroke patient’s gait patterns were slow and required excessive exertion; however, these patient’s legs were not well coordinated. Thus, increased foot support time and decreased gait speed in these patients with balance disorders were the risk of falls and increased anxiety.48 Combined with clinical analysis, stroke mainly occurs in the 60 to 70 years old, where the decline of body function inevitably leads to the FoF. Impaired balance can easily cause patients to fall and, thus, cause them to be aware of the surrounding environment and the safety of their activities, which eventually increases the patient’s psychological tension, worry and FoF.49 Therefore, it is vital to explore the relationship between FoF and body function in clinical practice using large-scale prospective studies.
In addition to the factors mentioned in the various studies, elements such as poststroke psychological factors, long-term sitting and quality of life research have been studied for the relationship with the FoF. Anxiety and depression (r=0.400), energy, mobility, self-care and upper extremity function of quality of life (Pearson’s correlation coefficients were r=−0.476; r=−0.615; r=−0.617; r=−0.507)19 were correlated with FoF. A significantly positive correlation was seen between FES-I and sitting time (r=0.579).50 The study on differences in gait and balance measures in patients with chronic stroke with the different levels of attention related to falls showed that patients with chronic strokes and slight concern about falling have better gait and balance capabilities than patients with high levels of concern.51 Therefore, these results are potentially clinically relevant and would be useful to study if reducing FoF can improve gait, quality of life, physical function and balance performance in these patients. Furthermore, it would also be useful to measure FoF as the assessment of psychological factors, quality of life and physical function in these patients. Although stroke itself is not a direct factor in causing the FoF, as a long-term chronic disease, it indicates that the patient’s body functions are further declining. Importantly, the treatment of long-term chronic diseases further declines or loses the patient’s self-efficacy and self-confidence in behavioural activities, which eventually leads to FoF. The decreases in self-esteem can directly cause depression, anxiety and limited self-care ability and affect FoF. Additionally, in the recovery stage of the first stroke, the walking function is the main factor affecting the occurrence of falls. Since most stroke patients have limb dysfunction, the need to assist in walking during the initial stage of recovery or within a certain period increases the risk of falls.
Furthermore, there is a particular aspect regarding the causal relationship between falling and FoF. Some studies have confirmed that FoF is an essential predictor of falls in patients with stroke,52–54 and several other studies have suggested that people who have experienced a fall were more likely to have FoF.55 56 A recent study has confirmed that the history of falls in the recent time was a good predictor for the FoF, but the FoF is a predictor of falls during follow-up only in the unadjusted model.57 In the current study, differences were observed among the included studies in terms of evaluation for the fall history. The fall history was defined as whether a fall was occurred in the past 6 months, within the past 1 year, or within 6 metres of walking. During these different periods, the probability of falling in stroke patients was different, which affects the likelihood of occurrence of FoF.58
Considering the global prevalence of stroke-related falls or FoF, this study provided evidence for developing appropriate preventable measures for decreasing the FoF risk in patients with stroke. The risk factors of FoF for stroke patients in Asia included marital status, social support status and payment methods for medical insurance59; However, current guidelines for stroke management provide no specific recommendations for psychological monitoring or the FoF management.60 Therefore, more studies are required for developing effective evaluation methods and treatment strategies against FoF among patients with stroke to improve their physical function, mental health and quality of life.
This meta-analysis had several significant findings. First, most of the included studies were relatively high quality, with robust evidence. Second, under the premise of a large sample size, the risk factors of falling fear in stroke patients were ensured by quantitative analysis. Hence, our findings may be more convincing compared with the individual studies. Additionally, the research data included in this study were adjusted, and the results of the data analysis were not affected by the patient’s baseline characteristics. We also explored the sources of heterogeneity using meta-regression if the analysis included more than two studies. We prespecified sample size and the proportion of women as the meta-regression variables because we considered that studies with smaller sample size and a larger proportion of women could have a larger impact on FoF.31 In the post hoc analyses, we also added age and SwePASS score as potential regressors because previous studies showed that older populations and smaller SwePASS scores could lead to a larger impact on FoF.31–33
Despite the above important findings, this study had some limitations. (1) Two of the included reports were cross-sectional studies, and, thus, the ability to hypothesise aetiology was weak, (2) all the included studies were observational studies, and, therefore, the role of confounding factors should be considered. However, due to the limited number of studies, a multivariate meta-analysis could not be performed to assess the robustness of our findings and analyse the effect size of multiple risk factors at the same time,61 (3) the effects of the patient’s inner anxiety and depression, as well as the motor function of the lower limbs on the risk of falling fear in stroke patients, have been reported in fewer studies. Therefore, the conclusions may vary for individual studies, (4) this meta-analysis only included English and Chinese studies; thus, it probably missed the relevant studies in other languages, which leads to biases in estimates in Western countries. However, there is currently no evidence suggesting that the meta-analysis of language limitations can lead to such bias.62 63 In the end, the analysis was based on the overall research level and not on personal data.
Conclusion
This study is the first systematic analysis for assessing the risk factors for FoF in patients with stroke, including the history of falls, walking aids, sociodemographic factors, physical characteristics and psychological factors. This study results suggest that women, impaired balance, mobility impairment, history of falls, walking aids, anxiety, depression, poor lower limb motor function and physical inactiveness might be associated with FoF in patients with stroke, especially impaired balance. In addition, the collective evidence was primarily consistent, and the effect size of FoF was large. A comprehensive analysis of these risk factors would help screen and differentiate patients at risk for FoF, thereby helping to prevent and optimise timely interventions.
Overall, there is a paucity of empirical data in this area. Many of the factors identified, in general, that population samples have not been studied in patients with stroke. In addition, other risk factors specific to patients with stroke (eg, gait speed and gait-related factors) need to be evaluated to identify patients with stroke at risk for FoF. Finally, researchers should explore how some variables (ie, anxiety and depression) interact with FoF and how to better protect patients with stroke from it. This intervention will reduce the personal and financial burden and promote these patients’ early recovery.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors QX and J-HP contributed equally to this work. Study design: QX, J-HP, X-MD. Analysis and interpretation of data: QX, J-HP, Y-BZ, LG. Drafting of the manuscript: QX, J-PZ, X-MD. Critical revision of the manuscript: Y-JS, X-MD, LG, X-LW, LM. X-MD accepted full responsibility for the work of the study, had access to the data, and controlled the decision to publish as the guarantor. All authors have read and approved the final version of the manuscript.
Funding This work was supported in part by the 2020 Cui Ying Science and Technology Plan Project-General Project, Lanzhou, Gansu, China (CY2020-MS19), Scientific Research Project of Health Industry in Gansu Province, China (GSWSHL2021-011).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.