Article Text

Abstract
Objectives Wearable motion sensors are used with increasing frequency in the evaluation of gait, function and physical activity within orthopaedics and sports medicine. The integration of wearable technology into the clinical pathway offers the ability to improve post-operative patient assessment beyond the scope of current, questionnaire-based patient-reported outcome measures. This scoping review assesses the current methodology and clinical application of accelerometers and inertial measurement units for the evaluation of patient activity and functional recovery following knee arthroplasty.
Design This is a systematically conducted scoping review following Joanna Briggs Institute methodology for scoping reviews and reported consulting the Preferred Reporting Items for Systematic Review and Meta-Analyses extension for scoping reviews. A protocol for this review is registered with the Open Science Framework (https://osf.io/rzg9q).
Data sources CINAHL, EMBASE, MEDLINE and Web of Science databases were searched for manuscripts published between 2008 and 2019.
Eligibility criteria We included clinical studies reporting the use of any combination of accelerometers, pedometers or inertial measurement units for patient assessment at any time point following knee arthroplasty.
Data extraction and synthesis Data extracted from manuscripts included patient demographics, sensor technology, testing protocol and sensor-based outcome variables.
Results 45 studies were identified, including 2076 knee arthroplasty patients, 620 patients with end-stage osteoarthritis and 449 healthy controls. Primary aims of the identified studies included functional assessment, physical activity monitoring and evaluation of knee instability. Methodology varied widely between studies, with inconsistency in reported sensor configuration, testing protocol and output variables.
Conclusions The use of wearable sensors in evaluation of knee arthroplasty procedures is becoming increasingly common and offers the potential to improve clinical understanding of recovery and rehabilitation. While current studies lack consistency, significant opportunity exists for the development of standardised measures and protocols for function and physical activity evaluation.
- accelerometry
- gait analysis
- systematic review
- knee arthroplasty
- physical activity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a comprehensive, systematic literature review following Joanna Briggs Institute methodology for scoping reviews.
The Preferred Reporting Items for Systematic Review and Meta-Analyses Extension for Scoping Reviews guidelines were followed for reporting clarity.
The use of wearable sensors was evaluated in subcategories based on the assessment functional analysis, physical activity and joint stability. Validation studies not directly addressing patient outcome were excluded from review based on the authors’ discretion.
Introduction
Patient-reported outcome measures (PROMs) are routinely used to evaluate the efficacy of knee arthroplasty procedures in terms of post-operative patient satisfaction, function and pain.1 2 PROMs are commonly implemented pre-operatively through patient questionnaires to establish a baseline measurement, and then again at 6 months post-operatively.3 Various forms of validated PROMs have been used throughout orthopaedic clinical practice and are effective in demonstrating overall patient improvement following surgical intervention.2 The effectiveness of PROMs, however, can be limited in some instances as a result of inherent ceiling effects1 4 as well as inaccurate and non-repeatable patient-reported post-operative activity.5 6 The Osteoarthritis Research Society International and Outcome Measures in Rheumatology and Clinical Trials advocate the use of functional outcomes for all randomised controlled trials of interventions after knee replacement.7 Traditional assessment has come through timed tests such as the Timed Up and Go or 6 min walk test; however, these are burdensome for participants and do not replicate their normal activity. Some researchers have suggested that PROMs incorporating patient function and activity measures may be the way forward in improved understanding of patient outcome and performance following unicompartmental knee arthroplasty (UKA) or total knee arthroplasty (TKA).8 9
Within the healthcare field, wearable technology is the application of data-recording transducers onto a person’s body or clothing to monitor measurable health indicators. Wearable technology is increasingly being used to perform gait analysis and to assess patient’s mobility and activity levels in orthopaedic and sports medicine, with wearable motion sensors generally consisting of an accelerometer measuring accelerations in 1, 2 or 3 degrees of freedom (df) to quantify limb or whole-body movement. More complex movement data can be collected from inertial measurement units (IMUs), sensors pairing accelerometers with gyroscopes and magnetometers to provide detailed analysis of limb movement and orientation within a spatial reference frame.
Several methodological considerations must be made during the implementation of wearable motion sensors in the study of surgical outcome. Body location, sampling rate, wear time and testing protocols are key aspects of sensor-based research which may affect the quality and reliability of data being collected.10–13 The manner in which these sensors have been deployed in knee arthroplasty research and clinical care has not been fully examined. This scoping review aims to assess the current methodology and clinical application of wearable sensors to evaluate patient recovery and functional outcomes following knee arthroplasty.
Methods
We conducted a scoping review following the Joanna Briggs Institute Methodology for JBI Scoping Reviews14 and consulted the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) Extension for Scoping Reviews checklist for reporting.15 The protocol is registered within the Open Science Framework (https://osf.io/rzg9q/). For inclusion within this review, manuscripts must report the use of wearable sensor technology for monitoring patient function, mobility, surgery effectiveness or joint stability, or to serve as the basis for the assessment of a questionnaire or other measure of physical activity and function. Included studies could be conducted in a hospital or home setting and must include post-operative data collection following any total or partial knee arthroplasty for end-stage osteoarthritis (OA). Explicit validation studies of wearable sensor technology and studies implementing the use of IMUs for robotic-assisted rehabilitation or surgical navigation were excluded, as those studies do not meet the primary aims of evaluating basic patient outcome. Full inclusion and exclusion screening criteria are presented in table 1.
Inclusion and exclusion criteria
To identify relevant studies, an electronic database literature search was conducted with assistance from outreach librarian Nia Roberts. Databases searched were CINAHL (1982 to present), EMBASE (1974 to present), MEDLINE (1950 to present) and Web of Science Core Collection (1945 to present) (see online supplementary table S1 for details on the strategies). Since wearable sensor technology is an emerging field benefiting from developments in miniaturisation and wireless data transfer, the literature search was designed to primarily capture the current use of modern wearable instrumentation. Thus, manuscripts published between January 2008 and June 2019 were considered. Additionally, reference lists of relevant articles were searched for additional appropriate inclusions. Systematic reviews were not included in the review but were also checked for potentially relevant references. On completion of the comprehensive searches, duplicate entries were removed through manual verification within Mendeley reference management software.
Supplemental material
Screening of manuscript titles and abstracts were conducted by two independent, blinded reviewers (SRS and GSB) through the use of the Rayyan systematic review web app.16 Prior to screening, reviewers discussed inclusion and exclusion criteria, while working through a calibration exercise of example titles and abstracts to ensure consistency between individuals. Following title and abstract review, SRS and GSB evaluated the subsequent full-text manuscripts for inclusion in the final review. Any disagreements following full-text assessment were discussed between reviewers. A third reviewer was available for consultation if no consensus could be reached.
Following the screening process, data from all included full-text manuscripts were collected within a data extraction spreadsheet by the first author (SRS) and then verified by GSB. Any inconsistencies were resolved by consensus. Data extracted from the manuscripts were categorised by patient demographics, technology, testing protocol and sensor-based outcome variables. Specifically, data were extracted to include the number of male and female participants in knee arthroplasty, end-stage OA or healthy control populations. The type of wearable sensor was recorded, including number of axes of motion recorded, as well as the use of accelerometers, gyroscopes, magnetometers and global positioning systems (GPS), and the reported data sampling rate for all sensor measurements. The number of sensors and body location was also recorded. For data charting purposes, manuscripts were divided into three distinct subgroups based on the primary aims of each study as follows: (1) studies with the primary aim of assessing functional or gait parameters, (2) physical activity studies with the primary aim of quantifying change in overall activity as a result of knee arthroplasty and (3) instability studies with the primary aim of assessing post-operative joint stability. The duration of free-living activity monitoring was extracted for all physical activity studies, as well as the pre-operative and post-operative time points when data were collected. Finally, sensor-based outcome variables were recorded to assess the specific metrics reported in each study.
Patient and public involvement
Patients and the public were not involved in any phase of this study.
Results
A PRISMA flow diagram17 detailing the results of the literature search and review is presented in figure 1. The searches yielded 346 records for title and abstract screening, of which 69 were assessed as full texts. Of these, 45 were included in the review. The 24 excluded studies lacked knee arthroplasty patients or stratified data, included too few study participants, were protocol or validation studies or deemed unrelated to the review question. While any type of knee arthroplasty for end-stage OA was included in the search, no studies evaluating patients following bi-compartmental, patellofemoral or other partial knee arthroplasty were identified.

Preferred Reporting Items for Systematic Review and Meta-Analyses literature review flow diagram.17
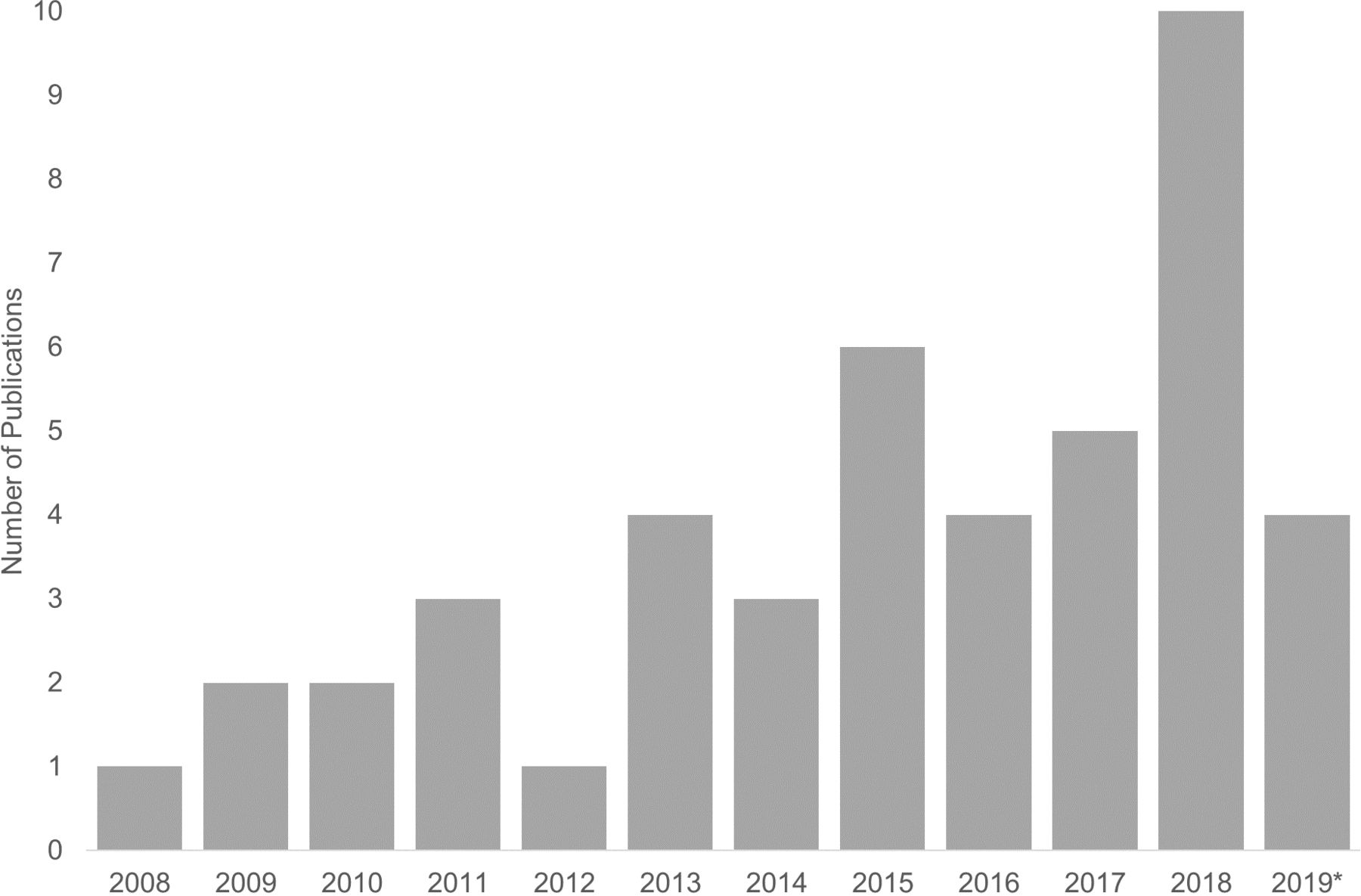
The use of wearable technology to assess outcome and effectiveness of TKA and UKA has increased over the period evaluated in this review. As shown in figure 2, an average of just 1–2 studies per year were published between 2008 and 2012. More recently there has been continued growth in the number of studies implementing wearable motion sensors entering the public record, with 10 wearable sensor-based studies focused on knee replacement in 2018. A full list of studies along with model and manufacturer of devices used can be found in online supplementary tables S2-S4.

{kind=link}
{kind=link}
The number of publications within this review by publication year (*2019 through June).
Functional assessment
Sixteen studies were included in the functional assessment subgroup (tables 2 and 3), comprising data collection on 451 TKA patients (57% female), mirroring the 43:57 male-to-female ratio within primary TKA across the UK.18 A single study included functional comparisons with 29 end-stage OA patients without knee replacement,19 while eight studies included comparative assessments with a total of 141 healthy control populations.8 19–25
Population and methods summary for functional assessment studies
Sensor summary for functional assessment studies
A triaxial accelerometer was the most commonly used sensor incorporated in the functional assessment subgroup, with 15 of 16 studies (94%)8 19–32 using the sensor alone or in combination with other instrumentation. Seven of the functional studies exclusively used triaxial accelerometers as the means for data collection during functional analysis.8 20–22 24 28 31 Three studies used IMUs with an integrated triaxial accelerometer and triaxial gyroscope,19 27 29 while three others recorded gait with a 9 df IMU integrating triaxial accelerometer, gyroscope and magnetometer.25 26 30 Storey et al 23 used a triaxial accelerometer for indoor gait analysis, but included two GPS watches for outdoor walking tests. Two studies by van Hemmert et al 32 33 incorporated the DynaPort ADL sensor system consisting of six uniaxial accelerometers, with one of those studies supplementing the DynaPort system with an additional triaxial accelerometer.32 Sensor sampling rate for data recording was varied across studies, ranging from below 50 Hz to 500 Hz and not directly reported in a third of studies.19 24 30 32 33 Body location for sensor placement was equally varied, with no more than seven studies sharing any one specific sensor placement.
Testing protocols within the function studies were generally consistent and primarily comprised gait analysis, with patients walking on a 10–20 m walkway or treadmill. Four studies20 22 32 33 used the DynaPort knee test protocol34 which includes a series of walking, stepping and lifting movements to mimic activities of daily living. Bolink et al 26 tested patients through a sit-to-stand protocol, while both Bolink et al and Christiansen et al 21 tested patients in stepping exercises. Most studies (13 studies, 81%)8 19–22 24–30 33 included pre-operative data collection with repeated tests at one or more time points up to 1-year post-operatively, most frequently up to 6 weeks after surgery. Three studies collected data at an unspecified point any time greater than 6 months post-operatively.23 31 32
The evaluation of gait symmetry and variability was the most common sensor-based outcome metric (eight studies, 50%),8 21 24 26 28 29 31 32 while dynamic range of motion was also commonly reported (six studies, 38%).19 25–27 29 30 A wide variety of spatiotemporal gait parameters were also reported, including varied combinations of walking speed,8 23 24 26 29 32 cadence,8 26 32 stride length,8 23 24 26 29 32 stride time,8 19 29 stance time,24 29 vertical displacement,8 32 swing power24 and foot fall.24 Three studies reported functional performance primarily based on a stand-alone function score.22 32 33 Other studies reported on gait function through a variety of other parameters including acceleration magnitudes,21 26 31 activity transitions,20 multiple aspects of dynamic range of motion19 26 27 29 and varied measures of gait symmetry, inefficiency and variability.8 21 24 26 28 29 31 32
Physical activity studies
Twenty-six studies were identified as primarily focusing on physical activity following knee arthroplasty (tables 4 and 5), including a total of 1490 patients (58% women). Five of those studies included comparisons with a total of 620 end-stage OA patients without a knee replacement,35–38 though 458 of those patients came from a single report.37 Three studies compared physical activity levels of knee replacement patients with a total of 272 healthy controls.35 39 40 Four studies also included physical activity from measures from total hip replacement patients for comparison with knee patients.41–44
Population and methods summary for physical activity studies
Technology summary for physical activity studies
Physical activity studies were consistent in the number of sensors implemented, with 21 studies (81%) using a single sensor for activity measurements.35–40 42 43 45–57 As technology and availability of wearable accelerometers has progressed, the type of sensor used has also changed. In studies published between 2008 and 2016, nine studies (69%)36 37 40 42 44 45 58–60 reported using a uniaxial accelerometer versus just three studies (23%)46 55 56 using a triaxial accelerometer. Conversely, in studies published in 2017–2019, eight studies (62%)35 38 47 49 50 53 54 57 reported using a triaxial accelerometer, while only three (23%)39 43 45 used a uniaxial accelerometer. Overall, three studies did not report the number of axes recorded,41 48 51 and most studies within this subgroup (73%)36 37 40–45 47 48 50–55 57 60 did not report the sampling rate at which data were collected. No standard frequency was observed within studies reporting sampling rate, as two studies collected data at 10 Hz,39 56 two at or near 30 Hz49 58 and three at 100 Hz.35 38 46 Accelerometers were mounted at hip or waist level, most commonly with an elastic strap, in half of the included physical activity studies.36–38 42 43 45–47 49 50 53 56 58 Seven studies positioned sensors on the thigh,35 39 41 44 48 58 60 four on the sternum,41 44 59 60 four on the lower leg,40 52 54 59 one on the foot59 and two on the wrist.51 57
All studies within this subgroup quantified physical activity based on free-living activity. Most commonly, free-living data was collected in 7-day sessions (13 studies, 50%),36–39 42 45–47 49 50 53 57 58 with 10 studies (43%)35 40 41 44 48 52 54 58–60 collecting data over shorter sessions (eg, 2–4 days). Four studies reported longitudinal activity metrics for longer time periods, with Hayashi et al 43 and Tsuji et al 56 reporting physical activity during post-operative hospitalisation for 8 and 14 days, respectively, while Luna et al 51 reported basic accelerometer counts for 20 days post-operatively and Taniguchi et al 55 asked patients maintain a daily step count log for 6 months following surgery. Two primary methodologies exist for sensor wear time. Fifteen studies (58%)35–38 42 43 45–48 53–55 58 59 instructed patients to wear the accelerometers during waking hours only, while 10 studies (43%)39–41 44 49 51 52 56 57 60 instructed patients to wear the accelerometers 24 hours/day.
Physical activity was measured at different time points primarily dependent on the type of studies being conducted. The longitudinal studies reviewed most frequently assessed physical activity within 1–2 weeks pre-operatively, and then subsequently near 6 weeks and 6 months post-operatively. Three longitudinal studies assessed physical activity up to 1 year post-operatively,47 52 58 while Vissers et al 44 reported physical activity up to 4 years follow-up. Cross-sectional studies were more varied, with some reporting at exact post-operative time points, while others evaluated patient activity at non-specific or broadly defined time points.36 37 45 46 The most commonly reported time points for activity analysis across all physical activity studies were pre-operatively (18 studies, 69%)25 39–42 44 45 49–54 56–60 and at 6 months post-operatively (12 studies, 46%).39 41 42 44 47 49 50 53 55 58–60
Sensor-based outcome variables within the physical activity studies varied considerably between studies, though not as widely as in the functional assessment subgroup. Reporting of step counts is the most commonly used measure of physical activity within the knee arthroplasty population and has been increasingly common within these studies, included in 9 of 12 (75%) studies35 38 39 43 47 49 50 54 57 from 2017 to 2019, compared with just 4 of 13 (31%) studies40 52 55 58 from 2008 to 2016. The amount of active and sedentary time (12 studies, 46%),38 40–42 44 48 49 52–54 59 60 quantification of time spent at different activity intensity levels (12 studies, 46%),38 40–42 44 48 49 52–54 59 60 and approximations of energy expenditure (10 studies, 38%)35–37 46 49 51 53 54 56 59 are also commonly used measures which provide another level of detail beyond basic step counting techniques. Three studies reported transitions between activities and bouts of activities.35 41 54
Instability studies
Three studies from the literature review used wearable sensors affixed to the operative tibia to examine overall joint instability following TKA.61–63 A total of 135 patients (69% women) were examined (table 6) with two studies including comparisons with a total of 36 healthy control patients.61 62 For instability measurement, Khan et al 61 and Soeno et al 63 used triaxial accelerometers, while Roberts et al 62 used an integrated IMU with triaxial gyroscope and triaxial magnetometer. Both Khan et al 61 and Roberts et al 62 recorded joint motion in patients at a minimum of 6 months post-operatively at a sampling rate of 100 Hz while patients performed stepping, sit-to-stand and walking protocols. Similarly, both studies compared joint stability between TKA patients and healthy controls. Khan et al 61 reported instability based on mean acceleration and distribution of acceleration frequencies, while Roberts et al 62 quantified means and ranges of acceleration and jerk parameters. Soeno et al 63 collected data on patients more than 1 year post-operatively at a sampling rate of 250 Hz while quantifying instability directional root mean square acceleration, comparing patients with and without self-reported subjective instability.
Population and technology summary for instability studies
Discussion
Wearable motion sensors are increasingly being used to assess patient function, physical activity and joint stability following knee arthroplasty. The use of IMUs and accelerometers allows clinicians and researchers the ability to track a broad scope of outcome measures as they relate to free-living activities outside of the clinical setting, with greater objectivity when compared with activity questionnaires. Currently, wearable technology has been most commonly used for pre-operative and post-operative comparisons at 6–12 months of follow-up, with less focus on early recovery and rehabilitation. No standard outcome measure or testing methodology has been established in wearable-based gait analysis or physical activity monitoring.
The use of wearable motion sensors for gait analysis is an attractive alternative to optical gait analysis for functional assessment of knee arthroplasty patients. Whereas optical gait analysis requires significant overhead with dedicated equipment and facilities, IMU gait analysis offers the potential of quick setup and data capture in a wide variety of gait protocols and environments. As is evident within the context of this review, however, current knee arthroplasty literature lacks consensus for testing method and performance measures of spatiotemporal gait parameters using wearable technology. Within optical gait analysis, standard reflective marker positions and testing protocols are well established in TKA research.64 65 Similar progress is needed in the implementation of standard measurements and performance-based tests for characterisation of patient function and recovery in sensor-based analysis. Testing protocols incorporating multiple activities, including those in which patients with knee OA find more challenging, may be more indicative measures of patients’ ability to return to participation in normal activities and overall function.66 In the authors’ clinical experience, many knee patients find activities such as navigating through a crowd of people to be one of the more difficult daily activities. Evaluation of more complex, real-world activities is perhaps where the benefit to integrating IMU-based gait analysis may be most valuable.
Functional assessment apart from gait analysis through simple clinical measures (eg, range of motion) can also be derived using IMUs. Ramkumar et al 30 recently reported a longitudinal study using two IMUs for monitoring knee flexion during daily exercise sessions up to 12 weeks post-operatively. Their method requires the patient to set up one IMU on the thigh and another on the proximal tibia across the operative joint, whereupon the patient performs daily regimented movements. Take-home IMU-based systems for functional assessment, as described by Ramkumar et al,30 are less prevalent than accelerometer-based systems for general activity monitoring as gyroscopes in 9 df IMUs have substantial power and data storage requirements.67 As a result, longitudinal functional assessment via IMU can be logistically difficult and requires a level of active interaction by the patient or caregiver for battery charging and initiation of data collection and transfer. Nevertheless, Ramkumar et al 30 demonstrate the feasibility of implementing longitudinal functional assessment of simple parameters, such as knee range of motion, into remote patient monitoring schemes.
Physical activity monitoring through accelerometry is a more established technique than IMU-based gait analysis. Accelerometers are less battery and memory intensive than IMUs and offer the possibility of extended data collection without active involvement by the patient or caregiver. To date, sensors have been typically deployed near the patient’s centre of mass for activity analysis, at the hip or back, to most accurately monitor patients’ overall movement.12 One of the more surprising findings of this review is the lack of research using wrist-worn activity monitors for evaluation of patients’ physical activity. While networks of IMUs may provide improved data quality when performing gait analysis with wearable sensors, a single wrist-based triaxial accelerometer is the most common method of personal, at-home activity tracking. Based on current market research, wrist-based monitors and smart watches account for 95% of commercial wearables sales.68 Outside of orthopaedics, a movement towards wrist-based sensors for physical activity monitoring has developed.12 This is likely to be a result of widespread public adoption of commercial fitness trackers and smartwatches,68 69 concerns of patient compliance with hip-based monitors,12 70 71 improved accuracy in wrist-based accelerometry72–75 and development of techniques for analysis of raw accelerometer data output.12 76 The largest deployment of population-based physical activity monitoring was the assessment of over 100 000 volunteers enrolled within the UK Biobank.77 The study used a triaxial accelerometer (AX3, Axivity) mounted on the participant’s dominant wrist to collect activity data continuously for 7 days.77 Presently, no studies have analysed physical activity from knee arthroplasty patients within the UK Biobank; however, significant research potential exists across a variety of fields and disciplines.
Within this review, most studies using wearable sensors in longitudinal cohort studies report incremental changes in physical activity from a pre-operative baseline to 6 weeks, 6 months or 12 months post-operatively. Within these studies, there has been conflicting evidence as to the level of improvement in physical activity levels of knee arthroplasty patients beyond their pre-operative baseline.49 78 Conversely, limited research has been conducted regarding the pattern of recovery based on physical activity and how the trajectory towards return to participation may inform clinicians of an individual patient’s early rehabilitation. Mapping early patient recovery may be a particularly valuable clinical application of activity monitoring after TKA, as patient questionnaires and self-reported patient function may not accurately represent true functional abilities in near-term follow-up.58 79 80 We identified only three studies employing a method for monitoring patients over a continuous period for more than 2 weeks following surgery. Recently orthopaedic manufacturer Zimmer Biomet along with corporate partner Apple began the largest prospective study to date involving wearable technology and joint arthroplasty, in the rollout of their Apple Watch myMobility platform.81 This multicentre prospective longitudinal cohort study will rely on iPhone and Apple Watch integration to continuously track patient step count, while exercise coaching following TKA, UKA and total hip arthroplasty in an aim will provide motivation during the recovery process. The primary and secondary outcomes of this study are based on 90-day post-operative questionnaire responses, incidence of manipulation under anaesthesia, standard function tests, satisfaction and healthcare costs, and not on patient activity measures. Nevertheless, this study demonstrates the capacity for activity monitoring and feedback through near-continuous data collection, as well as the continued emergence of wrist-worn devices as a preferred data collection site in post-operative activity studies.
As Thompson et al 82 have noted, opportunity exists for physical activity monitors to provide multidimensional metrics to fine-tune activity guidelines for specific patient populations. Current literature lacks depth as to the type of sensor-based outcome metric best suited for evaluation of post-operative recovery, and how to best provide feedback to the patient. Since physical activity is multidimensional, improved monitoring during early rehabilitation can be used to explore the rate of recovery, overall mobility and patient satisfaction based not only on the amount of activity achieved, but also on the nature and timing of that activity within early post-operative period. The establishment of an evidence-based target recovery curve could be used as a baseline during the entire rehabilitation process from which to identify positively or negatively trending patient outcomes. Feedback mechanisms could be established to encourage more, or less, of a specific type of activity based on the expected activity levels at the specific patient’s post-operative time. Recently, Panda et al reported the ability to differentiate oncological patients suffering post-operative complications through passive physical activity monitoring.83 As they have demonstrated, real-time monitoring of physical activity by means of a sensor paired with a data network could direct the clinical care team to patients exhibiting a suboptimal recovery pattern who might benefit from additional evaluation or follow-up. As Ramkumar et al 30 explored in their recent pilot study, remote monitoring of patient recovery also has the potential to reduce un-necessary in-person clinical follow-up visits if the clinical care team can remotely identify patients’ tracking along an established recovery trajectory.30
The use of accelerometers in instability studies seems to be a niche research area, but one that demonstrates the versatility of wearable motion sensors within post-operative care and research. The development of research techniques, such as the quantitative measurement of the subjective patient experience of joint instability, could be a valuable tool in the refinement of overall evaluation of surgical intervention. The application of wearable technology in the assessment of two competing implant designs, as Soeno et al 63 have done, adds another tool available in the effort to improve outcomes and overall patient satisfaction.
The authors acknowledge limitations to this scoping review. The use of wearable sensors for the assessment of knee arthroplasty patients is accelerating. Subsequently, several studies will likely be published between the completion and publication of this review. Since the use of wearable technology continues to be an emerging technique in knee arthroplasty patient assessment, particularly within the field of gait analysis, exclusion of validation studies based on their level of clinical inquiry was subject to the authors’ best judgement. However, this review focuses on usage of sensor-based patient care and reflects emerging techniques practically implemented into current clinical practice.
The goal of this review was to investigate key trends in wearable sensor research within the scope of TKA and UKA. The use of wearable sensors in knee arthroplasty research is increasing, with gait analysis and physical activity the two primary modes of investigation. Wearable sensors offer potential for the advancement of patient care to include bespoke rehabilitation and follow-up schedules based on remotely collected ambulatory monitoring of physical activity, range of motion and gait parameters within the patient’s free-living environment. In practice, this could result in fewer clinical visits for patients with on-target recovery markers and opportunities for early intervention in patients following a suboptimal recovery curve. The technology also offers a mechanism for patient coaching and encouragement for patients to reach targeted goals during rehabilitation. To fully realise the clinical potential of wearable technology for knee replacement patients, this review highlights the need for increased focus on early recovery as well as increased inter-study consistency through improved technical reporting and standardisation of sensor-based outcome metrics.
Acknowledgments
The authors would like to thank Nia Roberts and Shona Kirtley for their support developing literature review and data extraction procedures, and Aiden Doherty for support in manuscript review.
References
Footnotes
Contributors All authors contributed to this review and approved the final manuscript. SRS designed and conducted the search, reviewed articles and wrote the manuscript. GSB reviewed articles and edited the manuscript. SK supervised the study process and edited the manuscript. KB supervised the study process and edited the manuscript. MT provided systematic review training to SRS, supervised the study process and edited the manuscript. AJP conceived the study, supervised the study process and edited the manuscript.
Funding Student funding for both SS and GB was provided by the Clarendon Fund from the University of Oxford and Oxford University Press.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.