Article Text

Abstract
Objectives This study determined the knowledge, attitude and practice/behaviour of cardiovascular health in residents of a semiurban community of Nepal.
Design To increase the understanding of knowledge, attitude and practice/behaviour towards cardiovascular health, we conducted in-home interviews using a questionnaire based on the WHO STEPwise approach to surveillance and other resources, scoring all responses. We also recorded blood pressure and took anthropometric measurements.
Setting Our study was conducted as part of the Heart-Health-Associated Research and Dissemination in the Community project in the Jhaukhel-Duwakot Health Demographic Surveillance Site in two urbanising villages near Kathmandu.
Participants The study population included 777 respondents from six randomly selected clusters in both villages.
Results Seventy per cent of all participants were women and 26.9% lacked formal education. The burden of cardiovascular risk factors was high; 20.1% were current smokers, 43.3% exhibited low physical activity and 21.6% were hypertensive. Participants showed only poor knowledge of heart disease causes; 29.7% identified hypertension and 11% identified overweight and physical activity as causes, whereas only 2.2% identified high blood sugar as causative. Around 60% of respondents did not know any heart attack symptoms compared with 20% who knew 2–4 symptoms. Median percentage scores for knowledge, attitude and practice/behaviour were 79.3, 74.3 and 48, respectively. Nearly 44% of respondents had insufficient knowledge and less than 20% had highly satisfactory knowledge. Among those with highly satisfactory knowledge, only 14.7% had a highly satisfactory attitude and 19.5% and 13.9% had satisfactory and highly satisfactory practices, respectively.
Conclusions Our study demonstrates a gap between cardiovascular health knowledge, attitude and practice/behaviour in a semiurban community in a low-income nation, even among those already affected by cardiovascular disease.
- Public Health
- Preventive Medicine
- Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Article summary
Strengths and limitations of this study
-
This study is the first to extensively explore knowledge, attitude and behaviour/practice regarding cardiovascular health in Nepal and was conducted in a health demographic surveillance site which provides the logistic advantage of further follow-up and intervention.
-
Using prompted and unprompted questions in the same study illustrates the variation that may be obtained by these approaches.
-
Unintentional oversampling of women respondents yielded unsegregated gender-wise results that are more likely to represent knowledge, attitude and practice/behaviour in women.
Introduction
Non-communicable diseases (NCDs) pose increasingly important public health problems in low-income and middle-income countries (LMICs). In 2008, 80% of global NCD deaths occurred in LMICs;1 NCDs recently accounted for 7.9 million of 14.5 million deaths (54%) in Southeast Asia2 and were responsible for two of every three deaths (34.5 million) worldwide in 2010.3 Poverty, illiteracy, poor-health infrastructure and demographic transition, including increasing life expectancy, are major contributors to the rising burden of NCDs in LMICs. Other postulated causes include poor fetal and childhood nutrition.4 ,5 A similar pattern is evident in South Asian countries like Nepal, where NCDs currently occur more frequently than communicable diseases and behavioural risk factors such as tobacco smoking are high.6
Globally, cardiovascular diseases (CVDs) are responsible for one in four deaths (12.9 million).3 Eighty per cent of CVDs result from tobacco smoking, unhealthy diet, physical inactivity and harmful use of alcohol.7 The risk of all-cause mortality among individuals who score poorly in behavioural factors is fourfold higher than in those who score best.8 In high-income countries, declining CVD mortality is largely attributed to the reduction of behavioural risk factors.9 Underlying socioeconomic parameters and societal influences affect exposure and vulnerability to CVD risk factors. Therefore, surveillance of NCD risk factors should include social determinants of cardiovascular health.1 ,10 Currently, understanding the individual and social determinants of cardiovascular health behaviours is among the top 20 priority areas for NCD research in LMICs.11
As a precursor of favourable health behaviour, experts have advocated health literacy since community-based interventions began exploring the potential impact of behavioural changes on CVD.1 ,12 The WHO promotes public awareness of diet and physical activity as a ‘best buy’ to improve cardiovascular behaviour.9 However, achieving the desired health behaviour requires a deeper understanding of the underlying social context of disease.13 ,14 Hence, studies on knowledge, attitude and practice (KAP) increase our understanding of cardiovascular health literacy and community behaviour.15 Currently, such studies have been limited in South Asia.
Earlier studies report low levels of knowledge about heart attack16 and diabetes symptoms in Nepal.17 Nepal's high prevalence of underlying behavioural risk factors, particularly tobacco and alcohol consumption and poor cardiovascular health knowledge, is a matter of concern.18 Nationwide in Nepal, the age group 25+ exhibits fasting blood glucose of 5.5 mmol/L for men and 5.4 mmol/L for women, systolic blood pressure of 125.9 mm Hg and 126.6 mm Hg for men and women, respectively, and total cholesterol of 4.1 mmol/L (men) and 4.3 mmol/L (women).19
Currently, attempts to improve cardiovascular health knowledge and behaviour in Nepal focus mainly on campaigns that transmit information but pay little attention to the population's actual health literacy. We therefore undertook a community-based KAP study in the Jhaukhel-Duwakot Health-Demographic Surveillance Site (JD-HDSS) outside Kathmandu where NCDs, particularly CVDs, are the predominant cause of morbidity and mortality.20 Additionally, our pilot study in the Duwakot population demonstrated poor cardiovascular health knowledge.21 Our study is part of the Heart-Health Associated Research and Dissemination in the Community (HARDIC) project, which is the cardiovascular health component of JD-HDSS. In Nepalese, hardic means ‘heartily’ or ‘from the heart’. This paper reports the baseline results from HARDIC and is the first to conduct a detailed analysis of cardiovascular health KAP/behaviour in an urbanising community of Nepal.
Methods
Ethical considerations
The Nepal Health Research Council and the Institutional Review Board of Kathmandu Medical College approved this study. Following a pattern established at the outset of JD-HDSS, we consulted local leaders and sought their informal permission for HDSS activities. In addition, we periodically consulted with health and administrative authorities in both villages. All participants gave informed consent, and privacy was maintained during the interview process. To maintain confidentiality, all data were secured in the HDSS office. Computer data were accessible only to the research team. Although respondents received no monetary incentives, we provided a referral that included discounted consultation fees at Kathmandu Medical College or Nepal Medical College for self-reported illness and newly diagnosed hypertension.
Study site
We conducted our descriptive, community-based, cross-sectional study between September and November 2011 in the JD-HDSS of Bhaktapur district in the Kathmandu Valley, 13 km from Kathmandu. An earlier report described the establishment of the surveillance site.20
Study population and sample size
This study is the first step in the larger HARDIC project that will be conducted in the whole JD-HDSS. Duwakot and Jhaukhel each contain nine administrative wards and we randomly selected three wards from each village. Based on the JD-HDSS 2010 baseline census,20 we compiled a complete list of households containing adults aged 25–59 years in the selected wards. Next, we selected one adult, of either sex, from all interview households and surveyed 789 of 840 households (non-response rate=6.07%). We applied the Kish technique to select the respondent.22
Study tools
We structured the basic questionnaire and tailored it to site-specific responses in Nepal using the WHO-NCD STEPwise approach to surveillance (STEPS; STEP 1 and 2 questionnaires) for demographic information, behavioural and physical measurements23 and other sources for addressing knowledge, attitude and practice/behaviour issues.15 ,24–39 Responses to questions on cardiovascular health knowledge, attitude and practice/behaviour were given scores in order to compare and correlate the components. A detailed description of the scoring system is given as an online supplementary appendix to this article.
Interviewers
Twelve local female enumerators (two/ward) conducted the interviews. All enumerators had completed at least grade 10 in school. Supervisors included four public health graduates; a field co-ordinator with Master's and PhD degrees in public health; and two PhD students/authors (AV and URA).
Data collection
Interview process
The interviews were conducted at the participants’ homes. The initial part of the interview consisted of questions related to demographic profile. Questions then followed relating to knowledge of cardiovascular health (eg, causes and risk factors, warning signs and action for suspected heart attack); heart-healthy diet and disease prevention. The first two areas included unprompted (spontaneous, open-ended) and prompted (clues provided, close-ended) responses, and the latter two areas included only prompted responses. We asked respondents about their attitude towards different aspects of cardiovascular health: did they perceive themselves at risk for CVD? Did they think behaviour change would reduce their risk of developing CVD? The responses were recorded on a Likert scale (strongly agree, somewhat agree, do not know, somewhat disagree, strongly agree).
Behavioural factors
Behaviour-related questions were based on Step 1 of the WHO STEPS, which uses a questionnaire to collect data on risk factors.23 Our questions probed current and past smoking behaviour; smokeless tobacco; alcohol consumption in the last 30 days (current drinker) and drinking frequency among current drinkers. The physical activity section asked respondents to report the number of days and amount of time they participated in vigorous and moderate activities at work, leisure and travel. Additional practice and behavioural questions explored whether participants had engaged in any heart-friendly behaviour in the previous year and for what reason.
Physical measurements
Enumerators recorded anthropometric measurements (ie, weight, height, and waist and hip circumferences) according to the STEPs guidelines.23 Weight was measured to one decimal place using a Microlife BR-9201 Weighing Scale (Microlife AG Swiss Corporation, Widnau, Switzerland). Height and waist and hip circumferences were measured using non-stretchable tapes (Jonson Tapes Ltd, New Delhi, India). Blood pressure was determined digitally by Microlife BP 3AP1-3E (Microlife AG Swiss Corporation, Widnau, Switzerland). Enumerators recorded three readings for each respondent, taken at 5-min intervals. We averaged the readings to attain the final blood pressure measurements.
Diagnostic criteria for subclassification
Respondents with a known history of hypertension (diagnosed cases) and those diagnosed during the study according to the Joint National Committee-VII40 were termed as having ‘hypertension’.
Data management
Supervisors checked all completed questionnaires and, if necessary, asked enumerators to revisit households. After omitting incomplete questionnaires, we included 777 individuals in the analysis. Except for missing recordings for height, weight or blood pressure, the data reported in our KAP study covers all 777 respondents. We outsourced data entry to a team of data entry operators, public health graduates by qualification. Data were coded and entered in Epidata V.2.1.
Statistical analyses
Data were analysed with SPSS V.17.0 (IBM, Armonk, New York, USA) and STATA V.10.0 (StataCorp, Texas, USA). After calculating the Metabolic Equivalent of Task minutes/week, we grouped participants as highly active, moderately active or inactive (low physical activity) in accord with the STEPS manual.
For scoring KAP/behaviour questions and to compare and correlate the three components, we scored responses regarding KAP/behaviour for cardiovascular health. The maximum possible scores for KAP/behaviour were 53, 56 and 25, respectively. Further, total knowledge score was classified into the following five categories based on the quintile scores: ≤20% ‘highly insufficient’; 21–40% ‘insufficient’; 41–60% ‘sufficient’; 61–80% ‘satisfactory’; >80% ‘highly satisfactory’.41
Categorical data are presented as numbers and percentages, and continuous data as the median and inter-quartile range (IQR). KAP percentage scores are presented as the median. We used the χ2 test to compare proportions among demographic variables and the Mann-Whitney U test to compare scores from men and women. p<0.05 was considered to be statistically significant.
Cronbach's α, which measures question reliability, for the overall knowledge and attitude was 0.941 (range: 0.775–0.913) and 0.824 (range: 0.791–0.822), respectively. Cronbach's α for practice and behaviour ranged from low (0.257) for physical activity questions to high (0.929) for blood pressure measurements.
Results
Demographic characteristics and cardiovascular risk factors
Table 1 describes the sex-wise demographic characteristics of the respondents. Seventy per cent of all participants were women, and 25% lacked formal education. The median age (IQR) for male and female respondents was 40 (33–49) years and 38 (32–46) years, respectively. Two-thirds of the female respondents were housewives and three of five men were either serviceholders or self-employed. We have shown previously that 59.2% belonged to the upper-lower class.20
Demographic characteristics of the study population
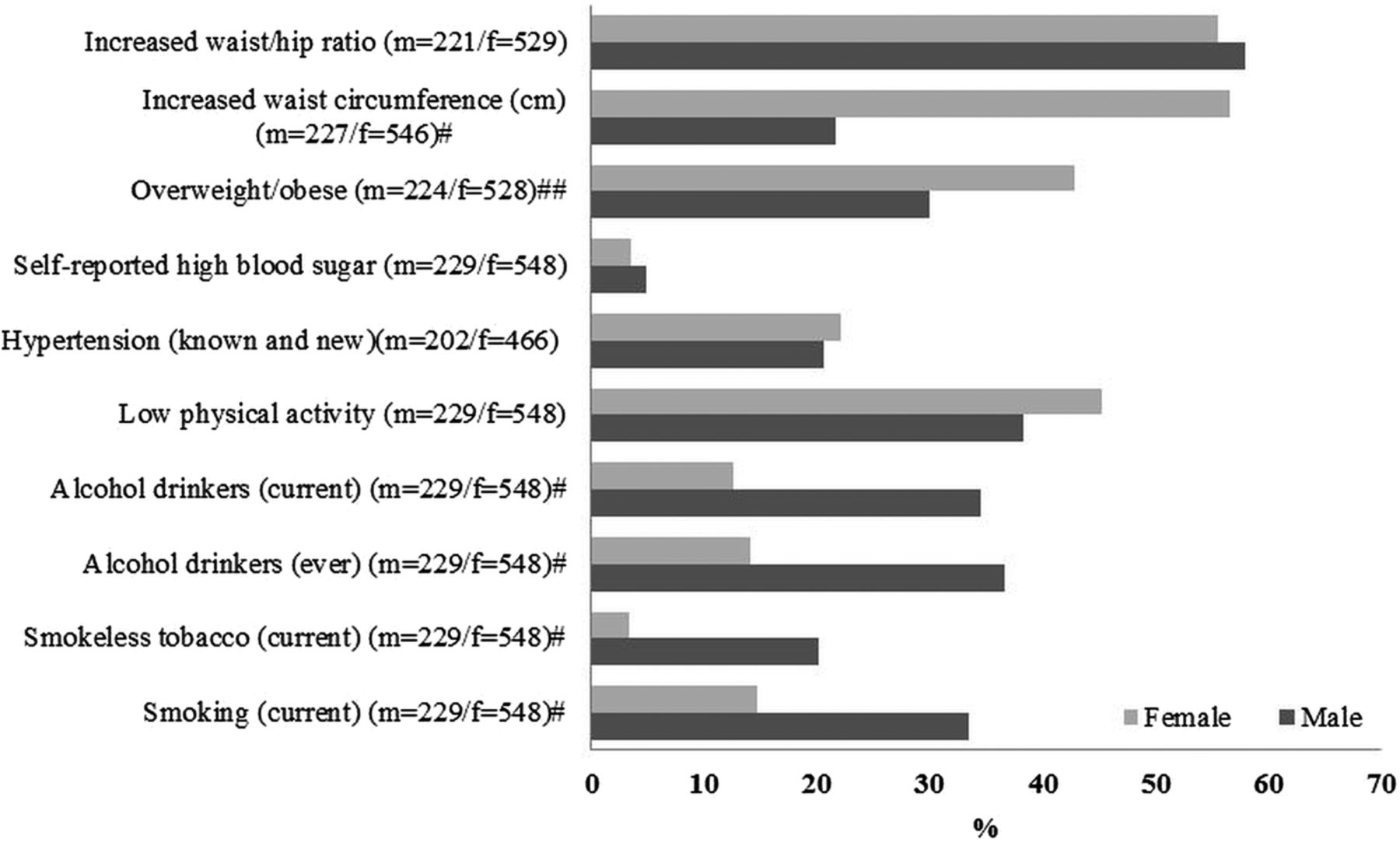
Figure 1 shows the sex-wise prevalence of cardiovascular risk factors in the study population. Overall, 3 in 10 respondents were past or current smokers and 1 in 5 respondents had consumed at least one alcoholic beverage in the previous month. More than 40% of the respondents reported low physical activity. The prevalence of known and newly diagnosed hypertension was 21.6%. As measured by body mass index (BMI), the prevalence of overweight and obesity was 29.7% and 9.4%, respectively. Abdominal obesity (ie, increased waist circumference and waist–hip ratio) was 46.3% and 56.3%, respectively. There was a statistically significant difference in the prevalence rate among men and women in smoking, smokeless tobacco use, alcohol intake, overweight/obesity and increased waist circumference.

{kind=link}
Sex-wise distribution of cardiovascular risk factor status in the study population. m, Number of males; f, number of females; # p<0.001, ## p<0.01 (χ2 tests). Risk factor categories were based on the WHO-NCD Risk Factor STEPS Survey manual.23 Current smokers included those who responded ‘yes’ to ‘Do you smoke?’ Past smokers included those who replied ‘yes’ to ‘Did you ever smoke in the past?’. ‘Ever drinkers’ included respondents who had ‘consumed a drink that contained alcohol ever in lifetime,’ and current drinkers included respondents who had ‘consumed alcohol within the previous month.’ The percentage of drinking frequency represents current drinkers who consumed at least one standard drink per occasion. Blood pressure data exclude respondents who did not submit to all three readings. Likewise, data for BMI, waist circumference and waist-hip ratio exclude respondents whose weight, height and waist and/or hip measurements were not taken. Increased waist circumference includes waist measurements of ≥80 cm (women) and ≥90 cm (men); increased waist–hip ratio is ≥0.85 (women) and ≥0.90 (men).
Knowledge towards CVD
Knowledge regarding causes and warning signs of heart disease
Table 2 shows unprompted responses for the perceived causes of heart diseases. The responses ranged from 1% for high blood sugar to 29.1% for smoking. The median percentage scores for men and women were 13.8% and 10.4%, respectively (p<0.001, Mann-Whitney U test). Younger respondents (<35 years) knew more than older participants (median 13.7% vs 10.3%, p=0.01). Respondents belonging to Brahmin, Newer and Chhetri ethnicities had less knowledge than those in the other caste/ethnicity group (median 13.8% vs 6.9%, p=0.001) (table 1). Respondents with high school or more education and working in government or non-government offices knew more than those with less education and in other employment situations (median 17.2% vs 10.34%, p=0.001).
Percentage of respondents citing various causes of cardiovascular disease and warning signs of heart attack
Table 2 also describes the warning signs of heart attack as perceived by the respondents. Around 60% of respondents did not know any of the heart attack signs. Among those who were familiar with those signs, nearly 50% of respondents knew only one sign, 37% knew any two signs, 11.42% knew any three signs and 2.53% knew four signs. The proportions of each warning sign told by the male and female respondents were not statistically different (p>0.05). The proportions of knowledge about warming signs were not statistically different in terms of age (χ2=3.39, p=0.49), caste/ethnicity (χ2=6.25, p=0.4) and education (χ2=5.50, p=0.53). Importantly, only 20% of respondents identified chest pain—the most prominent and important indicator of heart attack—as a symptom of heart attack.
Knowledge on action in case of a heart attack
When asked about what action the respondents would take for a suspected heart attack, more than 20% gave no response and 75% (81.2% men and 73% women, χ2=4.05, p=0.04) said they would immediately take the affected person to hospital. About 3% said that they would try home therapy, consult a traditional healer or stay home and wait for the symptoms to go away.
Knowledge on healthy foods for heart diseases
When asked to identify a particular heart-healthy food, most respondents identified green-leafy vegetables (94.6%) and fruit (92.1%). Furthermore, 22% thought salty food like chips and around 7% thought fried food or saturated fat (eg, ghee) are healthy foods.
Attitudes and practice towards CVD
Attitude towards heart health in an urbanising community
Table 3 describes opinions reflecting attitudes towards various aspects on heart diseases. Regarding lifestyle and preventive measures, 25% of men and 30% of women perceived themselves to be at risk of CVD. More than half of the respondents did not want to change their current lifestyle (64.6% men vs 55.4% women, p<0.01). Nearly 23% said that they ate more and would like to cut down; approximately 82% considered themselves to be overweight, the perceived proportion being significantly higher among men (p<0.05); nearly 32% believed that they did not have time to take care of themselves; and three-fifths did not think that changing their behaviour would lower their cardiovascular risk. Further, 25.3% of men and 27.2% of women thought that God or a higher power determined their health.
Responses to attitude-related questions on cardiovascular disease
Table 3 also describes the respondents’ opinions on various preventive aspects of heart health that would be helpful. Almost all respondents believed that increased access to fruits, vegetables and other healthy foods would be helpful. Nearly 9 in 10 respondents thought that greater access to indoor and outdoor public recreational facilities would be helpful. Four per cent of respondents did not believe that smoking bans would be helpful to reduce heart diseases. Eight in 10 male respondents believed that local volunteers should try to change any adverse health behaviours while nearly 9 in 10 women believed the same (p<0.01).
Practice towards heart diseases
Half of all the respondents had their blood pressure measured and 10% reported getting a diagnostic test for CVD in the previous year. About 60% attempted to reduce their consumption of unhealthy foods and 25% tried to lose weight or increase physical activity. Half of the smokers said that they had attempted to quit smoking.
When enumerators asked the respondents who reported one or more positive health behaviours the main reason for trying to change their lifestyle or practice/behaviour, the reasons given were: they wanted to feel better (70%); had seen, read or heard information (65.4%); did it for their family (45.9%); or were encouraged to do so by a healthcare professional (41.3%), family member (39%) or friend (31.8%). Other reasons for changing lifestyle or practice/behaviour included wanting to avoid taking medications (20.6%); a family member, relative or friend who developed CVD, became ill or died (16.5%); and developing possible cardiovascular symptoms (14.8%).
Comparison between level of knowledge, attitude and behaviour/practice
Overall, the average prompted knowledge of heart diseases (median 79.3%) was 11.5% lower than the average attitudes (median 67.8%) and nearly 31.1% higher than the average practices (median 48.2%). Next, the average level of attitude scores was nearly 19.6% higher than that for practices. Similarly, the average spontaneous knowledge of heart diseases (median 10.3%) was 57.5% lower than the average attitudes (median 67.8%) and nearly 40% lower than the average practices (median 48.18%).
Table 4 describes the level of KAP based on quintile scores. Regarding knowledge, 20.4% of the respondents had highly insufficient knowledge, 23.2% had insufficient knowledge, 22.6% had sufficient knowledge, 16.5% had satisfactory knowledge and 17.2% had highly satisfactory knowledge. Similarly, attitude levels were as follows: highly insufficient 20.6%, insufficient 26.9%; sufficient 15.4%; satisfactory 11.2% and highly satisfactory 19.8%. Regarding behaviour/practices, it was highly insufficient in 12.1% of the respondents, insufficient in 24.3%; sufficient in 22.7%; satisfactory in 27.5% and highly satisfactory in 13.4%. Among those with highly insufficient knowledge, 20.3% of them had highly satisfactory attitudes and 6.9% had highly satisfactory practices. Conversely, among the respondents with highly satisfactory knowledge, 14.7% had highly satisfactory attitude and 19.5% and 13.9% had satisfactory and highly satisfactory practices, respectively. Likewise, 1 in 10 respondents with satisfactory knowledge had a satisfactory attitude while 2 in 10 had a highly satisfactory attitude. Nearly 4 of 10 had satisfactory/highly satisfactory behaviour. As the level of knowledge increased, the highly satisfactory practice also increased from 6.9% to 13.4%. However, when the level of knowledge increased, the highly satisfactory attitude decreased from 20.3% to 14.7%.
Percentage distribution of the level of knowledge, attitude and behaviour/practice regarding cardiovascular health
Regarding attitude, among those with the level of attitudes of highly insufficient, 41.2% had satisfactory/highly satisfactory behaviour/practice. When the level of attitude was highly satisfactory, 35% had satisfactory/highly satisfactory practice. Similarly, when the attitude was sufficient, 25% had insufficient practice and nearly 41% had satisfactory practice. When the level of attitude increased, the proportion of those with highly satisfactory practice remained unchanged.
A comparison of male and female respondents showed no difference in the level of knowledge (χ2=4.4, p=0.4), attitudes (χ2=3.6, p=0.5) and practice (χ2=2.1, p=0.7). However, there were significant differences in the level of knowledge according to age (χ2=18.1, p=0.02), caste/ethnicity (χ2=43.8, p<0.001) and education level (χ2=48.7, p<0.001). In contrast, the level of attitude was not statistically significant for these variables (p>0.05). On the other hand, the level of practice was also statistically different according to age (χ2=18.7, p=0.01), caste/ethnicity (χ2=21.1; p=0.004) and educational status (χ2=45.7, p<0.001).
Respondents <35 years of age were more likely to have highly satisfactory knowledge (37.3% vs 29.2%) and practice (38.5% vs 19.2%) than those >45 years. Brahmins (30.5%) were more likely to have highly satisfactory knowledge than Newars (27.6%), Chhetris (20.4%) and others (21.5%). Regarding highly satisfactory practice, the proportion was highest among Brahmins (41.3%), followed by Chhetris (30.8%), Newars (17.3%) and others (10.6%). Those who had no formal schooling exhibited a higher proportion of highly satisfactory knowledge than those who had high school or more education (28.3% vs 24.6%, but highly satisfactory practice was low among them (12.5% vs 28.8%, data not shown).
Discussion
The present study is the first to conduct a detailed analysis of the relationship between KAP/health literacy and cardiovascular health in a semiurban setting near Kathmandu.
Cardiovascular risk factors are abundant in the study population
Our respondents showed a high burden of behavioural and biological risk factors. While the prevalence of tobacco smoking was similar to the national average, the alcohol consumption was lower.42 National figures on tobacco smoking and alcohol consumption for Bangladesh, Nepal, India and Pakistan show that current smoking of any tobacco product (age-standardised rate, both sexes) is 24%, 32%, 15% and 20%, respectively.19 The total adult (recorded and unrecorded) per capita consumption of pure alcohol according to the WHO-available projected estimates for 2008 indicates that consumption in Bangladesh, Nepal, India and Pakistan is 0.17, 2.42, 2.69 and 0.05 L of pure alcohol, respectively, over a calendar year.19 The numbers have been increasing in these countries over the last few years.19
In accord with our earlier review on obesity in Nepal, the effect of urbanisation is evident in low physical activity and overweight/obesity that exceeds the national average.21 ,42 The prevalence of hypertension in our study population is similar to the national average (22%) but less by about one-third than a study in Bhadrabas, a similar semiurban Kathmandu community,43 most probably due to the different age groups. The 2008 national reported age-standardised level of hypertension in Nepal is similar to levels in Bangladesh but lower than in Pakistan (38.6% and 39.5%, respectively) and higher than in India (35.2%).44 Self-reported prevalence of diabetes mellitus (3.9%) confirms the JD-HDSS baseline figure reported earlier.20
Knowledge of cardiovascular health is limited
Our study population showed low overall knowledge of the causes of CVD. Unprompted responses suggested that respondents identified behavioural factors (eg, smoking) more frequently than physiological causes (eg, hypertension). Other studies have reported similar findings for unprompted38 and prompted responses.33 Conversely, unhealthy diet, obesity and family history were common responses in Taiwan.31 In Vietnam, knowledge on the negative influence of tobacco smoking on stroke and heart attack is lower than general knowledge regarding health risks of active smoking and exposure to second-hand smoke.45
Many of our respondents also attributed CVD to environmental factors such as food hygiene and air pollution. Indeed, acute inflammatory reactions to air pollutants accelerate coronary atherosclerosis and trigger arrhythmia or myocardial infarction.46 Unlike the Strong Heart Study39 in American populations, our results did not exhibit a higher probability of knowledge of a risk factor in persons who have that risk factor, demonstrating poor cardiovascular health literacy even among those already affected.
Similar to Pakistan,15 a large majority (60%) of our respondents could not identify even one heart attack symptom. However, similar to an earlier study in Nepal,16 6–22% of individuals in our demographic subsets recognised chest pain as a symptom, which is less compared with 60% of Vietnamese Americans who spontaneously mentioned chest pain.47 Importantly, two-thirds of heart attack patients delayed their arrival at a Karachi hospital because they did not recognise heart attack symptoms.15 Similar to a previous study,18 three quarters of our respondents believed they would immediately take a suspected heart attack patient to a hospital, but one-fifth did not answer the question or opted instead for home therapy or traditional healing. Combined with our earlier finding of not knowing heart attack symptoms, this lack of knowledge about appropriate action underscores the need to educate the Nepalese population about this issue. In contrast, 85% of Vietnamese Americans knew that they should immediately call 911 if they suspected a heart attack.45 Despite inadequate knowledge about the causes of CVD, our respondents were much better informed about preventive measures. This finding concurs with the perception level of American women,35 probably because enumerators asked prompted questions in this section of the questionnaire. In Taiwan, only 25% of respondents thought that CVD was preventable and 50% were ‘not sure.’31
Inappropriate attitude towards cardiovascular health
In contrast to their opinion that behavioural modifications can prevent CVD, most of our respondents did not consider themselves at risk and did not want to alter their lifestyle. This may be explained by the Health Belief Model.48 Others have described a similarly optimistic bias.49 Risk indicators (eg, number of cigarettes smoked; death of a parent due to CVD and self-assessment of blood pressure, weight and cholesterol levels) account for a 24% variance in perceived risk.49 The likelihood of perceiving oneself at higher risk increases when the presence of a risk factor is known.31 However, respondents often underestimate their cardiovascular risk.49
Attempts for better cardiovascular health practice/behaviour
Compared with Nepal's national average (69%), only half of our respondents underwent blood pressure measurement in the previous year.42 Ninety per cent of the known hypertensive population had their blood pressure under control, exceeding the 6% and 9.5% control rate reported in two other suburban Kathmandu studies43 ,50 and an urban study in Eastern Nepal (58.5%).51 Half of the smokers reported here that they had tried to quit smoking. Our questionnaire did not explore whether they had actually quit and did not identify the barriers against quitting, information that might be important for public health. The theory of reasoned action48 argues that intention is a critical component of healthy behaviour. Although confirming that the genuineness of intention is difficult, such intention may provide an opportunity for public health intervention. Importantly, we identified our respondents’ reasons for attempting positive health behaviour. Many constructs of the Health Belief Model,48 such as perceived benefit (‘wanted to feel better’), cues to action (‘encouraged by a health professional, etc’) and fear (‘death of a family member, etc ’), appear to affect behavioural decisions.
Influence of gender
Although women were unintentionally oversampled, our analysis includes a gender-wise stratification and we presented data separately whenever we observed marked gender differences. In our study, more men than women smoked tobacco or drank alcohol. The prevalence of hypertension and self-reported diabetes was similar in both groups. On the other hand, low physical activity and obesity were higher in the women. Although men had better knowledge of heart disease, their attitude was similar to those reported by women. However, more women than men strongly agreed that their health was ultimately determined by God or a higher power. Female gender is usually significantly related to good knowledge of CVD.52 One major factor for the gender discrepancy in our study is that more women (33.2%) than men (11.8%) lacked formal education, which in itself is alarming. In fact, illiteracy is one of the main risk factors along with behavioural factors in rural/urban Asian Indian women.53
Effect of other sociodemographic variables on KAP
Age-wise, KAP/behaviour scores decreased around 4% from the youngest to the oldest age group. An earlier study reported a higher level of knowledge among young respondents.36 Interestingly, a study in adolescents reported a very poor level of cardiovascular knowledge.54 Otherwise, knowledge levels rise linearly from childhood until middle age, when the level starts to plateau.55 In our study, better-educated respondents ate more fruit and consumed less tobacco and alcohol, but they also reported less physical activity and more hypertension. The highest education category (high school or more) scored higher than the lowest category (no formal schooling) but only by 3–8%. Other studies observed a consistent link between better KAP scores and higher education.31 ,36 ,52 ,56 Occupation-wise, employed respondents knew more about biological causes (eg, high blood pressure, diabetes and high cholesterol), possibly due to more education, wider exposure to information and better access to screening and treatment. A Canadian study reported similar findings.36
Prompted versus unprompted responses
Although we used unprompted responses to evaluate general knowledge, we used prompted responses to calculate scores, thus providing a denominator (‘full marks’) to calculate median score %. In other settings, KAP studies have variably used prompted33 ,39 ,47 ,57 or unprompted questions,16 ,31 ,38 while some studies used both.35 Other studies did not identify their chosen method.32 Although the accuracy of prompted versus unprompted questions in knowledge assessment has been a topic of debate, prompted questions confer a higher level of knowledge.58 When we analysed knowledge responses based on prompted responses, the percentage of correct answers increased drastically. The psychological explanation is that respondents must simply ‘recognise’ answers to prompted questions, but they must engage in the more difficult mental process of ‘recalling’ answers to unprompted questions.59 We believe that unprompted responses more accurately reflect knowledge level because they emerge from a thought process that involves respondents' knowledge, experience and perception regarding a specific issue.
Comparison between levels of KAP towards CVD
The findings of the study indicate that there is a gap in knowledge attitude and practices. The poor relation between KAP scores was unsurprising because a linear relationship between variables may not exist in cardiovascular health (eg, highly satisfactory knowledge=high satisfactory attitude and behaviour). Valente argued that each of six possible behaviour change models contains a varying order of KAP/behaviour and that a population can be described in terms of the percentage that fits into each model.60 This implies that no universal intervention can improve the cardiovascular health KAP of every individual in a community. The challenge lies in identifying individuals who fit into different linear models. Furthermore, health behaviour theories (eg, social cognitive theory and the theory of reasoned action)48 suggest that knowledge and attitude are only two components of the pathways that lead to behaviour. Constructs (eg, self-efficacy) and other personal and environmental factors (in social cognitive theory) and perceived behavioural control, subjective norms and ultimately intention (in the theory of reasoned action) play crucial roles in shaping one's health behaviour.48
Study limitations
Women were unintentionally oversampled (72.7%), although the male : female ratio of the study population was 1 : 1.15.20 Women were more likely to be available in the households when enumerators visited as most of the women in our study were housewives. The age-range was limited to 25–59 years as the age groups 60–64 and 70–74 years only constituted 1–2% of the total JD-HDSS population. Most of the respondents belonged to the caste/ethnic groups Brahmin, Chhetri and Newar, which are not representative of all caste/ethnic groups in Nepal. Further, respondents' and interviewers' mood, as well as place and time of interview, may affect the study. There is also the possibility of recall bias when questions are asked about history of CVD risk factors.
Conclusion
Our community-based cross-sectional HARDIC study demonstrated poor knowledge, inappropriate attitude and highly adverse behaviour regarding cardiovascular health in a semiurban community of Nepal even among those already affected by CVD. We aimed to determine a baseline KAP in the community to aid the planning of health promotion activities. Our results show the potential and possibility that community health promotion can improve cardiovascular health literacy.
Acknowledgments
The authors are grateful to the study participants. We acknowledge all enumerators; field supervisors (Rachana Shrestha, Vishal Bhandari, Chandra Shova Khaitu and Shova Poudel); and our field coordinator, Professor Dr Muni Raj Chhetri. We thank scientific editor Karen Williams (Kwills Editing Services, Weymouth, MA, USA) for providing professional English-language editing of this article.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors AV designed the study, performed statistical analysis and drafted the manuscript. URA performed statistical analysis and revised the manuscript. AK helped design the study and provided critical revision of the manuscript. All authors have read and approved the final manuscript.
-
Funding This study was supported by grants from the Wilhelm & Martina Lundgren's Foundation (vet1-367/2011 and vet1-379/2012) and the University of Gothenburg, Sweden through a ‘Global University’ grant (A11 0524/09).
-
Competing interests None.
-
Ethics approval Nepal Health Research Council.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.